A Framework for Clinical e-Science
330 likes | 455 Views
A Framework for Clinical e-Science. Welcome to our Industrial Steering Group Partners. Today’s Meeting. Get to know each other Tell you something about CLEF Start to find out How we can best work together What you would find of most value What you have that would help us

A Framework for Clinical e-Science
E N D
Presentation Transcript
A Framework for Clinical e-Science Welcome to our Industrial Steering Group Partners
Today’s Meeting • Get to know each other • Tell you something about CLEF • Start to find out • How we can best work together • What you would find of most value • What you have that would help us • Who else we should be talking to
University of Sheffield University College London University of Brighton Judge Institute Royal Marsden NHS Trust University of Manchester Project Participants
Management & Policy Evidence based health care Clinical Practice, Audit & Governance Clinical trials recruitment A Convergence of Need Post genomic research Need for more and better clinical information
STOP STOP STOP STOP Problems with Accessing Clinical information ? Much useful clinical information is still only in free text (clinic letters) that computers can’t read Medicolegal, ethical and practical barriers prevent large scale data sharing between institutions UNION SELECT COUNT Patient_ID FROM Patients, Narrative, Diagnosis, Intervention WHERE ((Patients.Patient_ID=Narrative.Patient_ID AND Patients.Patient_ID=Diagnosis.Patient_ID AND Patients.Patient_ID=Intervention.Patient_ID) AND (Diagnosis.Name=“cancer” AND Diagnosis.Locus=“head of the pancreas” AND Intervention.Name= NOT “pancreaticduodenectomy”)AND (Patients.YearOfDeath BETWEEN Diagnosis.Year AND Diagnosis.Year+5)GROUP BY Patients.Date_of_death Query interfaces for interrogating databases about temporal relationships are complex Date-ordered view of record is too comprehensive and only records what happened, not why SetA.Def {All unique patient & experience[[event.surgery:pancreaticoduodenectomy treats[event.problem:cancer hasLocus[head of pancreas]]] & timedAt[time_point starts[time_interval:more than 5 years endedBy[time_point timeOf[now]]]]]} SetB.Def {SetA & experience[event.intervention.drug administration hasDrug[gemcitabine] & NOT timedAt[(time_point similarTimeAs[time_point timeOf[event.intervention.drug administration hasDrug[chemotherapy drug]])] & occursBefore[time_point timeOf[event.intervention.drug administration hasDrug[gemcitabine] occursJustBefore [time_point timeOf [event.intervention.Radiotherapy]]]} SetC.Def {SetA minus SetB} SetD.Def {SetB & experience[event.problem:death & timedAt[time_point starts[time_interval:less than 5 years & endedBy[time_ point timeOf[event.surgery:pancreaticoduodenectomy treats[event.problem:cancer hasLocus[head of pancreas]]]]} SetE.Def {SetC & experience[event.problem:death & timedAt[time_point starts[time_interval:less than 5 years & endedBy[time_ point timeOf[event.surgery:pancreaticoduodenectomy treats[event.problem:cancer hasLocus[head of pancreas]]]]} Query.Def {(Size(SetB) - Size(SetD)) / Size(SetB)} Query.Def {(Size(SetC) - Size(SetE)) / Size(SetC)} UNION SELECT COUNT Patient_ID FROM Patients, Narrative, Diagnosis, Intervention WHERE ((Patients.Patient_ID=Narrative.Patient_IDAND Patients.Patient_ID=Diagnosis.Patient_ID AND Patients.Patient_ID= Intervention.Patient_ID) AND (Diagnosis.Name=“cancer” AND Diagnosis.Locus=“head of the pancreas” AND Intervention.Name=“pancreaticduodenectomy”) AND (Patients.YearOfDeath BETWEEN Diagnosis.Year AND Diagnosis.Year+5) GROUP BY Patients.Date_of_death)
Why start with cancer ? ‘Huge variations in cancer care’ BBC News 22nd May 2003 ‘Wheat may prevent colon cancer’ BBC News 23rd February 2002 ‘Breast cancer at record levels’ BBC News 2nd June 2003 Major priority for NHS and Research ‘Direct-to-Consumer Marketing of Genetic Tests for Cancer: Buyer Beware’ Journal of Clinical Oncology 21st July 2003 High public interest and concern ‘Vitamin cocktail cuts cancer deaths’ BBC News 4th August 2003 Clinical care and gene research strongly linked in cancer ‘Vitamin D boosts cancer treatment’ BBC News 14th June 2003 ‘Gene to halt ovarian cancer found’ New Scientist 23rd June 2003 Cancer patient EPR is information rich >100 letters per patient over lifetime ‘Gene test may show if cancer will respond to chemotherapy’ The Independent 1st August 2003 ‘Scientists stunned as pioneering British research cuts death rate by 30 per cent’ The Independent 1st June 2003
Ethical oversight committee GRID CLEF’s Goals • Collect clinical information from multiple sites • Analyse, structure and integrate it • Make it available using GRID tools (e.g. myGrid) • To authorised clinicians and e-Health scientists • In a secure and ethical collaborative framework
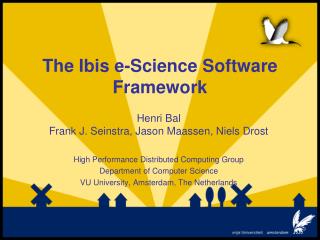
Knowledgeenrichment Hazardmonitoring Integrate &Aggregate PseudonymisedRepository ExtractInformation Ethical oversightcommittee Depersonalise Chronicle PrivacyEnhancementTechnologies Summarise & FormulateQueries Construct‘Chronicle’ Individual Summaries & Queries Reidentify By Hospital Researchers reqired to notify possible reidentification risks ArchitectureOutline …and federated in a single secure data repository …and integrated with structured information (e.g. lab tests, theatre records)… …and also contribute additional information (e.g. adding never stated diagnosis of anaemia if blood results suggest it) Significant clinical information identified in text (e.g. diagnoses, drugs, clinical findings etc)… Information extraction informed by data already in repository Less obvious identifiers removed from text (e.g. occupation) Clinical e-Scientists connected by Grid …query the repository for e.g. numbers of patients with specific diseases. …and ‘Chronicle’ view added to repository References reconstructed between information (e.g. Problem X was discovered during Investigation Y)… Pseudonymise In Hospital Obvious patient names & identifiers masked by source hospital All interactions between e-Scientists and repository approved and monitored by ethical oversight committee. …but answers are monitored to prevent reidentification of patients by cross reference or data mining. Clinicians from original hospital can view summaries and query the repository… Hospital exports its electronic records of regular clinical practice …and reidentify specific patients, only with permission
Knowledgeenrichment Knowledgeenrichment Hazardmonitoring Hazardmonitoring Integrate &Aggregate Integrate &Aggregate PseudonymisedRepository PseudonymisedRepository ExtractInformation ExtractInformation Ethical oversightcommittee Ethical oversightcommittee Depersonalise Depersonalise Chronicle Chronicle PrivacyEnhancementTechnologies PrivacyEnhancementTechnologies Summarise & FormulateQueries Summarise & FormulateQueries Construct‘Chronicle’ Construct‘Chronicle’ Pseudonymise In Hospital Pseudonymise In Hospital Individual Summaries & Queries Individual Summaries & Queries Reidentify By Hospital Reidentify By Hospital ArchitectureOutline Data Access Cycle Data Acquisition Cycle
CLEF Data Cycle Data Acquisition
Reports dictated For hospital use: ROYAL MARSDEN NHS TRUST - PATIENT CASE NOTE 324A621F:MRS Dorothy Smith DOB: 12/05/44 21, Park Crescent Basingstoke B12 Q13 16 Dec 1992 Seen in General Surgical This lady who has had a mastectomy and left open capsulotomy and removal of her prosthesis was seen by me in the clinic today on behalf of Mr Peterson. She has extensive bony lymphoedema in her left arm which does not seem to be getting any better although she is more or less reconciled to the problem. The original problem was that she complained of shooting pain in the direction of ulna nerve and although there does not seem to be any evidence of local, regional or distant recurrence the pain itself warrants management in a pain clinic. Mrs Smith could be seen in the pain clinic at the Marsden but as this would involve a lot of travelling would like to be treated nearer her home. I wonder whether it would be possible for you to investigate if there is a pain clinic available at Basingstoke as I am sure Dotty could be treated and benefit from its management. I have otherwise arranged for her to be seen in the clinic again in a year's time. There are no signs of recurrence at this time. Mr Thomas Partridge
Date of birth reduced to year Clinic date blurredpreserving sequence Obvious mentions of patient name or hospital name removed Overt identifying information removed in hospital & ID replaced by CLEF Entry Key Carer pseudonymised Pseudonymisation at hospital ROYAL MARSDEN NHS TRUST - PATIENT CASE NOTE 324A621F:MRS Dorothy Smith DOB: 12/05/44 21, Park Crescent Basingstoke B12 Q13 16 Dec 1992 Seen in General Surgical This lady who has had a mastectomy and left open capsulotomy and removal of her prosthesis was seen by me in the clinic today on behalf of Mr Peterson. She has extensive bony lymphoedema in her left arm which does not seem to be getting any better although she is more or less reconciled to the problem. The original problem was that she complained of shooting pain in the direction of ulna nerve and although there does not seem to be any evidence of local, regional or distant recurrence the pain itself warrants management in a pain clinic. Mrs Smith could be seen in the pain clinic at the Marsden but as this would involve a lot of travelling would like to be treated nearer her home. I wonder whether it would be possible for you to investigate if there is a pain clinic available at Basingstoke as I am sure Dotty could be treated and benefit from its management. I have otherwise arranged for her to be seen in the clinic again in a year's time. There are no signs of recurrence at this time. Mr Thomas Partridge ROYAL MARSDEN ##### ####### 324A621F:MRS Dorothy Smith ########:######### ####### 12/05/44 1944 21, Park Crescent Basingstoke B12 Q13 CLEF-RMH-Entry-Key: 52A4F6DB2B46E 16 Dec 1992 AB 1992 Mrs Smith XXXXXXXXX Marsden XXXXXXX Basingstoke XXXXXXXXXXX Mr Thomas Partridge 5213A4F612F1
Carer name spotted & pseudonymised Nick-name “Dotty”spotted by language software & removed Depersonalisation by CLEF Language Technology… ##### ####### NHS TRUST - PATIENT CASE NOTE ########:######### ####### DOB: 1944CLEF-RMH-Entry-Key: 52A4F6DB2B46E AB 1992 Seen in General Surgical This lady who has had a mastectomy and left open capsulotomy and removal of her prosthesis was seen by me in the clinic today on behalf of Mr Peterson. She has extensive bony lymphoedema in her left arm which does not seem to be getting any better although she is more or less reconciled to the problem. The original problem was that she complained of shooting pain in the direction of ulna nerve and although there does not seem to be any evidence of local, regional or distant recurrence the pain itself warrants management in a pain clinic. XXXXXXXXX could be seen in the pain clinic at the XXXXXXX but as this would involve a lot of travelling would like to be treated nearer her home. I wonder whether it would be possible for you to investigate if there is a pain clinic available at XXXXXXXXXXX as I am sure Dotty could be treated and benefit from its management. I have otherwise arranged for her to be seen in the clinic again in a year's time. There are no signs of recurrence at this time. 5213A4F612F1 Non-obvious identifyinginformation removedusing languagetechnology XXXXXXXXXXX XXXXX
General Surgical left open capsulotomy mastectomy removal of her prosthesis today bonylymphoedema left arm shooting pain in the direction of ulna nerve local, regional or distant pain recurrence pain clinic management pain clinic pain clinic management a year’s time clinic no signs of recurrence at this time Extraction of keyinformation from text ##### ####### NHS TRUST - PATIENT CASE NOTE ########:######### ####### DOB: 1944 CLEF-RMH-Entry-Key: 52A4F6DB2B46E AB 1992 Seen in General Surgical This lady who has had a mastectomy and left open capsulotomy and removal of her prosthesis was seen by me in the clinic today on behalf of XXXXXXXXXXX. She has extensive bony lymphoedema in her left arm which does not seem to be getting any better although she is more or less reconciled to the problem. The original problem was that she complained of shooting pain in the direction of ulna nerve and although there does not seem to be any evidence of local, regional or distant recurrence the pain itself warrants management in a pain clinic. XXXXXXXXX could be seen in the pain clinic at the XXXXXXX but as this would involve a lot of travelling would like to be treated nearer her home. I wonder whether it would be possible for you to investigate if there is a pain clinic available at XXXXXXXXXXX as I am sure XXXXX could be treated and benefit from its management. I have otherwise arranged for her to be seen in the clinic again in a year's time. There are no signs of recurrence at this time. 5213A4F612F1 Information Extraction identifies events and relationships between them from the text, based on templates & knowledge resources Interventions Problems Problem Site Locations Time
left open capsulotomy General Surgical General Surgical management left open capsulotomy management mastectomy left open capsulotomy mastectomy mastectomy removal of her prosthesis removal of her prosthesis today removal of her prosthesis today bonylymphoedema no signs of recurrence bonylymphoedema bonylymphoedema left arm left arm pain shooting pain in the recurrence shooting pain in the direction of ulna nerve shooting pain in the direction of ulna nerve local, regional or distant direction of ulna nerve local, regional or distant pain recurrence pain local, regional or distant recurrence pain clinic management left arm pain clinic pain clinic pain clinic management General Surgical pain clinic pain clinic radiology, pathology and other narrative reports pain clinic pain clinic pain clinic management clinic a year’s time today management clinic a year’s time a year’s time clinic no signs of recurrence no signs of recurrence at this time at this time at this time Information from laboratory and pharmacy systems Extraction of keyinformation into Data Structure Extracted information collected… across multiple documents Interventions Problems Problem Site Locations Time
management pain clinic Extraction of keyinformation into Data Structure Information extraction also collates repeated reporting of same event left open capsulotomy management Interventions management mastectomy removal of her prosthesis no signs of recurrence recurrence Problems bonylymphoedema pain shooting pain in the direction of ulna nerve Problem Site local, regional or distant left arm General Surgical pain clinic Locations pain clinic Provenance of information linked to original texts… pain clinic clinic today Time a year’s time at this time ..including multiple source documents
left open capsulotomy management Interventions mastectomy removal of her prosthesis no signs of recurrence evidence recurrence Problems bonylymphoedema pain shooting pain in the direction of ulna nerve Problem Site local, regional or distant left arm General Surgical pain clinic Locations pain clinic pain clinic today Time a year’s time at this time The CLEFChronicle Including the links to original texts, this is the CLEF Chronicle Internal links between events added by information extraction: What happened & why ? What was done & why ? mastectomy caused_by bonylymphoedema
Patient reidentifiable only by source hospital, with permission Hospital EPR EPR Drugs Refer Tools Help CLEF-RMH-Entry-Key: 52A4F6DB2B46EFemale 66 with radiation induced leukaemia since 1931 Onset age 63. Thirty three appointments to date. Problems: Aplastic anaemia, cataract, asthenia Tx:imatinibMeds: unclear CLEF-RMH-Entry-Key: 52A4F6DB2B46EFemale 66 with radiation induced leukaemia since 1931 Onset age 63. Thirty three appointments to date. Problems: Aplastic anaemia, cataract, asthenia Tx:imatinibMeds: unclear Staging CT Protocol 354 Drugs Appt Results Letters BP Summary for top of screen/page for all patient interactions Haem Chem Immu Bact Xray ECG USS Summarisation forPatient Care Very brief summaryof chronicle for recordheader and front sheet is available to source hospital … CLEF-RMH-Entry-Key: 52A4F6DB2B46E Maria Sklodowska-Curie can be incorporated within the hospital system 12.10.20 Coryza: chest NAD: reassure13.10.20 URTI: wheezy: amoxycillin20.10.20 Anxiety: lump under arm: staging scan24.10.21 PEFR : 300 :10.11.21 PEFR : 400: CXR requested12.11.21 CXR Basal Consolidation: : erythromycin27.11.21 : Chest clear :07.03.30 Depression: recurrence: Paroxetine19.04.30 WCC OK01.06.31 : : rpt Rx paroxetine18.10.31 Pain L arm: : coproxamol03.03.31 Viral URTI: PEFR 350: salbutamol04.03.34 WCCAbnormal : :30.05.34 : BP, ECG NAD :
CLEF Data Cycle Data Access
CLEF e-Scientist LOGIN Login Query OMIM Exit User ID: Password: Users of this site are bound by CLEF Privacy Policy CLEF Security Policy Data Protection Act Medical Records Act Use is monitored by the CLEF Ethics oversight board. CLEF User ID CL-00236F Authorisation LEVEL 2 Possible physical identification of users by biometric readers or smartcard Digital certificates issued per session Access for e-Scientists Cumulative repository is made accessible for remote querying by e-Scientists… ******** ********** Identity Confirmed …under control of oversight committee. Once user is authenticated, level of access authority is retrieved from oversight committee.
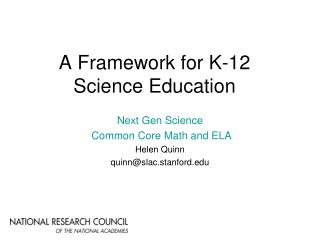
CLEF WYSIWYM Query Writer – L2 Login Query OMIM Exit Relevant Subjects Patients with [this type of tumour] at [this site] AND [another characteristic]. Treatment Profiles Patients who received [radiotherapy] [daily], compared with patients who received [radiotherapy] [every other day] and those who received [no radiotherapy]. Patients who received [this type of treatment], compared with patients who received [this type of treatment]. Outcome Measures Percentage of patients [alive] after [1 year] and after [2 years] and after [5 years]. Percentage of patients in [this condition] after [this interval of time]. Feedback Text Result of running query displayed as generated text… Generated text confirms the nature of the query For all patients with adenocarcinoma of the breast, compare the survival at 1, 2 and 5 years for those patients who had daily radiotherapy, those who had radiotherapy on alternate days, and those who had no radiotherapy Links out to other bioscience resources e.g. OMIM, PubMed, Gene Ontology …or graphically E-Scientist formulates queries e-Scientists construct queries using structured query writer Patients with [this type of carcinoma ] at [this site] Patients with [adenocarcinoma] at [this site] Patients with [adenocarcinoma] of [this laterality] of [this part] of [breast] adenocarcinomabasal carcinomasquamous carcinomatransitional carcinoma carcinoma carcinoma-in-situsarcomaneuroma bladderblood brain breastcervixcolonendometriumkidneylarynxlunglymphnodeoesophagusovarypancreas prostaterectumskinstomachtestistongue AND [this genetic marker]. AND [BRCA1 (OMIM 113705)]. nothing else this clinical stage this grade this genetic marker--------------------------- this symptom has had this treatment this complication QUERY RESULT1792 patients diagnosed with adenocarcinoma of the breast were found. 788 had radiotherapy daily, 513 had it on alternate days and 491 had no radiotherapy. After 5 years, 20% (n=158) of patients who had a daily treatment were alive. After 5 years, 10% (n=49) who had alternate day treatment were alive. After 5 years, 5% (n=27) of the patients who had no treatment were alive.
CLEF WYSIWYM Query Writer CLEF Patient Chronicle Viewer – L2 Login Query OMIM Exit Exit 1974 Grade III infiltrating ductal carcinoma left breast 7/22 sampled nodes positive Radical Mastectomy Left Breast Insertion Left Breast Prosthesis MEFUP Chemotherapy 1982/3 Recurrence Left supraclavicular nodes Excision biopsy of nodes Radiotherapy 1992 Replacement of Left Breast Prosthesis Removal of replacement to left breast prosthesis 1994 Recurrence inside chest (confirmed biopsy) VAC Chemotherapy aborted (toxicity) Radiotherapy completed L5/S1 degeneration Left phrenic nerve paralysis 1996 Multiple pulmonary emboli Post-radiation fibrosis left upper lung Prior rib fractures Frontal lobe ischaemic atrophy Teflon injection vocal cord 1997 Recurrence in chest Pleural effusions VAC Chemotherapy 6 cycles 1998 Recurrence in chest Radiotherapy Normal Left Shoulder Xray 1999 No evidence of recurrence Congestive cardiac failure Died June 1999 Relevant Subjects [Male] patients with [adenocarcinoma] of of [this laterality] of [this part] of [breast] AND [age] at [diagnosis] was [less than 30]. Treatment Profiles Patients who received [radiotherapy] [daily], compared with patients who received [radiotherapy] [every other day] and those who received [no radiotherapy]. Outcome Measures Percentage of patients [alive] after [1 year] and after [2 years] and after [5 years]. Queries on small patient groups are blocked or the figures blurred. Textual summary of CLEF Chronicle for patient #17 Graphical ‘time line’ view of CLEF Chronicle Privacy Enhancement& authorisation # 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Queries logged,threats to confidentiality monitored. [Female] patients with [adenocarcinoma] of of [this laterality] of [this part] of [breast] malefemale With special authorisation researchers may examine individual records in anonymised form. 17 QUERY RESULT1792 patients diagnosed with adenocarcinoma of the breast were found. 788 had radiotherapy daily, 513 had it on alternate days and 491 had no radiotherapy. After 5 years, 20% (n=158) of patients who had a daily treatment were alive. After 5 years, 10% (n=49) who had alternate day treatment were alive. After 5 years, 5% (n=27) of the patients who had no treatment were alive. WARNINGLess than 20 male patients diagnosed with adenocarcinoma of the breast were found. Further subanalysis on small groups increases the risk that a patient may be identifiable. Your CLEF security authorisation does not permit your query to be processed.
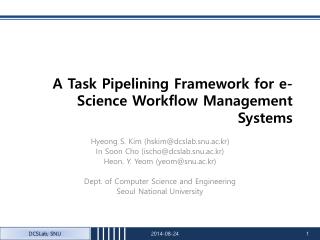
Data Summarisation & Visualisation R R R R Grade III infiltrating ductal carcinoma left breast Died RADIO CHEMO TAMOXIFEN ARIMIDEX Nodes Liver Spleen Kidney Bone Nodes Liver Spleen Kidney Bone Staging CT S S S S S S S S S S S S S T1>N1>M0 T1N3cM0 T1>N3cM1 >Stage IIA Stage IIIc Stage IV Recurrence 1975 1980 1985 1990 1995 2000
Lab # 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 CLEF WYSIWYM Query Writer CLEF Patient Chronicle Viewer – L1 Login Query OMIM Exit Exit Relevant Subjects [Female] patients with [adenocarcinoma] of of [this laterality] of [this part] of [breast] AND [age] at [diagnosis] was [less than 30]. Treatment Profiles Patients who received [radiotherapy] [daily], compared with patients who received [radiotherapy] [every other day] and those who received [no radiotherapy]. 17 Outcome Measures Percentage of patients [alive] after [1 year] and after [2 years] and after [5 years]. QUERY RESULT1792 patients diagnosed with adenocarcinoma of the breast were found. 788 had radiotherapy daily, 513 had it on alternate days and 491 had no radiotherapy. After 5 years, 20% (n=158) of patients who had a daily treatment were alive. After 5 years, 10% (n=49) who had alternate day treatment were alive. After 5 years, 5% (n=27) of the patients who had no treatment were alive. Higher security authorisation, more detail visible… Hazard Monitoring Report Hazard ROYAL MARSDEN NHS TRUST - PATIENT CASE NOTE ########:######### #######DOB: 1944CLEF-RMH-Entry-Key: 52A4F6DB2B46E AD 1997 Seen in Pain Clinic Dear XXXXX, Thankyou for referring XXXXXXXXX to me. I know her quite well, as she is captain of my local ladies’ golf team. As you say, her tumour is responding satisfactorily at the moment to Arimidex. She does not complain of any severe symptoms now, except continuing lymphoedema of the arm. I will see her again in 3 months time. 5213A4F612F4 Automated anonymisation unlikely to be perfect. Users can report possible hazards they encounter.
Lab Lab # 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Report Hazard CLEF WYSIWYM Query Writer CLEF Knowledge Editor – L1 CLEF Patient Chronicle Viewer – L1 Exit Exit Login Query OMIM Exit Hb Hb Relevant Subjects [Female] patients with [adenocarcinoma] of of [this laterality] of [this part] of [breast] AND [age] at [diagnosis] was [less than 30]. + Treatment Profiles 0 5 10 15 20 0 5 10 15 20 Patients who received [radiotherapy] [daily], compared with patients who received [radiotherapy] [every other day] and those who received [no radiotherapy]. WCC Evidence 17 + Outcome Measures Percentage of patients [alive] after [1 year] and after [2 years] and after [5 years]. 0 5 10 15 20 LFT QUERY RESULT1792 patients diagnosed with adenocarcinoma of the breast were found. 788 had radiotherapy daily, 513 had it on alternate days and 491 had no radiotherapy. After 5 years, 20% (n=158) of patients who had a daily treatment were alive. After 5 years, 10% (n=49) who had alternate day treatment were alive. After 5 years, 5% (n=27) of the patients who had no treatment were alive. Event: + 0 5 10 15 20 Period of clinical anaemia, not recorded in chronicle Yes No Cancel Knowledge Enrichment Authorised users can also augment chronicle with additional information. + ID(5627) ID(5645) ID(5685) NB. Research access to depersonalised narratives will be highly restricted anaemia Problem Type: diagnosisDate: 6F to 9B UMLS CUI:C0002871
Knowledge Resources • Internal knowledge sources • Clinical significance – what’s clinically obvious” • “only osteoporosis” “No bony metastases” • Leukopaenia possible cause to stop treatment • Tamoxifen is used in breast cancer may cause menopausal symptoms sometimes treated with HRT • Linguistic resources and corpora • External knowledge sources • Pubmed, UMLS, other literature … • OMIM, GO, other databases… • Standards • HL7, CEN EHR, NCICB CaCore, …
Links & Related projects • Bioinformatics • GO, GONG, MGED, EBI • Post-genomic research & cancer • NCRI/NTRAC/NCTR/NCRN • BioBank • NHS & Healthcare • Cancer Networks & National Programme • International • NCICB, Mouse/Human Anatomy projects • E-Science & Standards • myGrid, CO-ODE/HyOntUse, ESNW, DTI, Semantic Web/Grid • HL7, CEN TC251, ISO TC215 • Semantic Mining NoE in 6th Framework
Deliverables • Privacy policies and framework • A steering group hopefully in collaboration with others • Information extraction • Clinical information from semi-parallel texts from parallel records • EHR/Chronicle/Repository • Specification and demonstrator of integrated populated • Workbench and Language Generation • Demonstration useful and usable interface for clinical bioscientist to access repository • Query methods for specification longitudinal chronicle • E-Science Implementation • Technical • Knowledge, metadata standards • Tools from CO-ODE, myGrid, E-Science
Year 1 Year 2 Year 3 Design Prototype Revise & Integrate Project Plan from 20K ft Policy & ethicsInformation flowInternal links External links Integrated Workbench &Privacy Enhancement WorkbenchPrototype Populated integratedRepository/Chronicles Repository/Chronicles architecture & simulation Robust Info Extraction /depersonalisation Info Extraction /depersonalisation demo Links to external knowledge & standards Internal Knowledge resources Integration, E-Science Web services Basic Engineering & architecture Vision& Plan first joined up demonstration Demonstrator & Evaluation
Empowering the e-Scientist Removing barriers to data sharing Enriching clinical knowledge bases Thank you for coming www.clinical-escience.org 2003- 2005