Download
1 / 62
680 likes | 1.32k Views
Liver Cancer Treatment. . Liver Cancer Treatment. Surgical Resection Liver Transplantation Radiation Therapy Radiofrequenzy Ablation Cryosurgery Local Chemotherapy Percutaneous Ethanol Injection Systemic Chemotherapy. . Liver Cancer Treatment. Surgical Resection

E N D
Liver Cancer Treatment Surgical Resection Liver Transplantation Radiation Therapy Radiofrequenzy Ablation Cryosurgery Local Chemotherapy Percutaneous Ethanol Injection Systemic Chemotherapy
Liver Cancer Treatment Surgical Resection Liver Transplantation Radiation Therapy Radiofrequenzy Ablation Cryosurgery Local Chemotherapy Percutaneous Ethanol Injection Systemic Chemotherapy
Liver Cancer Treatment Surgical Resection Surgical resection may be a curative treatment for HCC But… …only 10% - 30% of patients with HCC are eligible for surgical resection because their pre-existing liver disease limits the regenerative capacity of their liver
Liver Cancer Treatment Surgical Resection In secondary liver cancer the 5 year survival after resection is between 20 and 40% , compared to 0% without resection. In HCC survival rates can be up to 75% after 5 years.
Liver Cancer Treatment Surgical Resection Absolute contraindications to resection of metastatic liver cancer are • Presence of extra hepatic metastasis • Inability to remove all hepatic disease In resected cancer patients with metastatic disease recurrence has occurred in 50% to 75% of the patients and remains the most important problem.
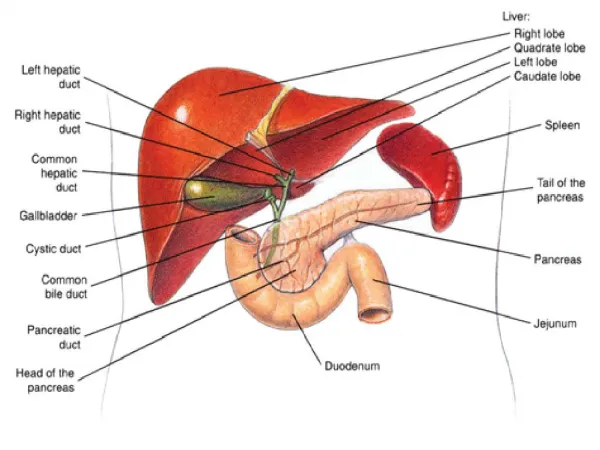
IX I VII VIII II III V IV portal vein VI Liver Cancer Treatment Anatomic Liver Resections
Liver Cancer Treatment In summary the limiting factors for a surgical resection of primary and secondary liver tumours are: • Remaining liver function • Number of tumour nodules (usually 3 or less) • Proximity or involvement of major hepatic vascular structures • Number of lobes affected (usually 1 only) • Tumour size (remaining liver function)
Liver Cancer Treatment Surgical Resection - Complications Intraoperative complications are: • Blood loss Postoperative complications are: • Liver failure • Ascites • Pleural effusions • Intraperitoneal infection • Major bile leak • Gastrointestinal bleeding
Liver Cancer Treatment Surgical Resection Liver Transplantation Radiation Therapy Radiofrequenzy Ablation Cryosurgery Local Chemotherapy Percutaneous Ethanol Injection Systemic Chemotherapy
Liver Cancer Treatment Liver Transplantation Transplantation for hepatic malignancies is indicated in the setting of either unresectable lesion(s), or coexistent cirrhosis resulting in both inadequate hepatic reserve and prohibitive portal hypertension
Liver Cancer Treatment Liver Transplantation Limitations: • Not all patients are eligible for transplantation • Availability of donor organs • Patients require lifelong immunosupression • Contraindicated in patients with secondary liver cancer R.L. Jenkis et al., Cancer Chemother Pharmacol 1989: 23: 104-109
Liver Cancer Treatment Liver Transplantation Survival data for patients with HCC undergoing liver transplantation: • 49% at one year • 37% at two years • 30% at three years R.L. Jenkis et al., Cancer Chemother Pharmacol 1989: 23: 104-109
Liver Cancer Treatment Surgical Resection Liver Transplantation Radiation Therapy Radiofrequenzy Ablation Cryosurgery Local Chemotherapy Percutaneous Ethanol Injection Systemic Chemotherapy
Liver Cancer Treatment Radiation Therapy The use of radiotherapy is limited as the liver does not tolerate large doses (above 35Gy). Nevertheless radiotherapy has a useful role in palliation of pain, nausea and vomiting.
Liver Cancer Treatment Surgical Resection Liver Transplantation Radiation Therapy Radiofrequenzy Ablation Cryosurgery Local Chemotherapy Percutaneous Ethanol Injection Systemic Chemotherapy
Liver Cancer Treatment Radiofrequency Ablation The radiofrequency ablation uses heat to destroy an entire tumour with minimal damage to adjacent vital structures. Radiofrequency is used as a source of thermal energy
Liver Cancer Treatment Radiofrequency Ablation - Procedure 3 parallel electrodes Multiple electrode array Thin needles are placed under imaging guidance into the tumour
Liver Cancer Treatment Radiofrequency Ablation - Procedure The needles are connected to a radiofrequency generator and function as an electrode
Liver Cancer Treatment Radiofrequency Ablation - Procedure Coagulation necrosis During the procedure a temperature of 500C to 1000C is maintained throughout the entire target volume The field of coagulation should include a 0.5 to 1cm margin of normal tissue
Liver Cancer Treatment Radiofrequency Ablation Limitations: • Not practicable for multiple lesions • Tumours in vascular environments • Only small tumours suitable (<3-4cm) • Relatively new technique • Limited number of studies published
abandoned Liver Cancer Treatment Surgical Resection Liver Transplantation Radiation Therapy Radiofrequenzy Ablation Cryosurgery Local Chemotherapy Percutaneous Ethanol Injection Systemic Chemotherapy
abandoned Liver Cancer Treatment Cryosurgery The cryosurgery uses subzero temperatures to destroy an entire tumour with minimal damage to adjacent vital structures. The terms cryosurgery, cryoablation and cryotherapy are interchangeable
abandoned Liver Cancer Treatment Cryosurgery versus conventional surgery or Cryosurgery can treat • bilobar disease • as many as 8 or 10 lesions • tumours adjacent to major vessels
abandoned Liver Cancer Treatment Cryosurgery In cryosurgery tumour cells are exposed to temperatures below -20°C for at least one minute This is generally lethal to living cells because: • Ice crystals damage cell plasma membrane • Ice crystals create a grinding effect • Small arterioles and venules are destroyed
abandoned Liver Cancer Treatment Cryosurgery Procedure: • The operative exposure is similar to liver resection • Cryoprobes are placed within the tumour centers • The probes are flushed with cryogen • Tip temperatures of -100°C are achieved • The freeze front is monitored by ultrasound • Aim is to freeze the whole tumour plus 1cm margin
abandoned Liver Cancer Treatment Cryosurgery Limitations: With this technique, patients with primary and secondary liver cancer can be treated if • the tumour size is less than 6cm • less than 50% cumulative liver volume is affected
abandoned Liver Cancer Treatment Cryosurgery Outcome: HCC with a tumour size less than 5cm 1 year survival 92.2% 3 year survival 75.5% 5 year survival 47.8% Colorectal metastasis (mean diameter 4.4cm) 1 year survival 82.4% 3 year survival 32.3% 5 year survival 13.4%
Liver Cancer Treatment Surgical Resection Liver Transplantation Radiation Therapy Radiofrequenzy Ablation Cryosurgery Local Chemotherapy Percutaneous Ethanol Injection Systemic Chemotherapy
Liver Cancer Treatment Local Chemotherapy There are two different approaches to local chemotherapy treatment: Transcatheter Arterial Chemoembolization (TACE) Hepatic Artery Infusional Chemotherapy (HAC or HAI)
Liver Cancer Treatment Local Chemotherapy There are two different approaches to local chemotherapy treatment: Transcatheter Arterial Chemoembolization (TACE) Hepatic Artery Infusional Chemotherapy (HAC or HAI)
Liver Cancer Treatment Transcatheter Arterial Chemoembolization (TACE) TACE aims to deliver high doses of a chemotherapeutic drug directly to the tumour and to simultaneously enhance the effect by embolization of the tumour vascularization The chemotherapeutic drug plus the embolic agent are injected via a hepatic artery catheter
Liver Cancer Treatment Transcatheter Arterial Chemoembolization (TACE) The major component is Lipiodol, which is iodized poppy seed oil Common chemotherapeutic agents are Doxorubicin, Cisplatin and Mitomycin C Other embolic agents like polyvinyl alcohol (PVA), gel foam, coils and degradable microspheres are also used
Liver Cancer Treatment Transcatheter Arterial Chemoembolization (TACE) Proposed effect of Lipiodol: • Enhanced accumulation in and around tumours • May enter tumour cells and induce death • Occlusive to tumour vascularity Less than 0.2ml/kg of Lipiodol are regarded as a safe dose. If of the whole liver needs to be embolized, 10-20ml are used. The normal dose is around 1ml per cm tumour diameter
Liver Cancer Treatment Transcatheter Arterial Chemoembolization (TACE) Advantages versus systemic chemotherapy: • Delivery of higher doses to the tumour • Less systemic side effects • Embolization cuts tumour off essential nutrients • Embolization enhances dwell time of drug
Liver Cancer Treatment Transcatheter Arterial Chemoembolization (TACE) Indications: • Unresectable HCC • Unresectable metastasis • Reduction of progression • Downsize tumour before resection Major Contraindications: • Extrahepatic disease • Poor liver function • Large arteriovenous shunting • Hepatic encephalopathy
Liver Cancer Treatment Transcatheter Arterial Chemoembolization (TACE) Patient workup: • Imaging (CT, MRT) • Labs • Angiography Procedure: Installation of the highly viscous TACE mixture via a hepatic artery catheter. Almost always a repeated treatment is necessary.
Liver Cancer Treatment Transcatheter Arterial Chemoembolization (TACE) Complications: • Post embolization syndrome • Acute progressive hepatic insuffiency (APHI) • Pulmonary oil embolism • Liver abscess • Cholecystitis • Non-target embolization of the gut • Gastrointestinal bleeding • Others
Liver Cancer Treatment Transcatheter Arterial Chemoembolization (TACE) Outcome: HCC Colorectal metastasis 1 year survival 54-88% 2 year survival 33-64% 3 year survival 18-51% 5 year survival <6% 1 year survival 78% 2 year survival 35% 3 year survival 15% In general the outcome is hard to quantify in a meta-analysis as many different protocols are used by different groups
Liver Cancer Treatment Local Chemotherapy There are two different approaches to local chemotherapy treatment: Transcatheter Arterial Chemoembolization (TACE) Hepatic Artery Infusional Chemotherapy (HAC or HAI)
Liver Cancer Treatment Hepatic Artery Infusional Chemotherapy (HAC/HAI) Like TACE, HAI (HAC) aims to deliver high doses of a chemotherapeutic drug directly to the tumour To achieve this, a drug is used which is highly extracted by the liver during the first pass with a short systemic half life time This is drug is usually Floxuridine(FUDR)
Liver Cancer Treatment Hepatic Artery Infusional Chemotherapy (HAC/HAI) The chemotherapeutic drug is automatically delivered by an implanted pump which pumps it directly into the hepatic artery
Liver Cancer Treatment Hepatic Artery Infusional Chemotherapy (HAC/HAI) Complications: • Surgical complications (pump placement) • Acute gastric or duodenal ulcers • Catheter or hepatic artery thrombosis (10%) • Septic complications • Biliary sclerosis (20%)
Liver Cancer Treatment Hepatic Artery Infusional Chemotherapy (HAC/HAI) Outcome: There are no good survival data available. Nevertheless this technique is regarded as efficient with response rates around 50% (42-62). One source mentions a 2 year survival rate of 47%
Liver Cancer Treatment Surgical Resection Liver Transplantation Radiation Therapy Radiofrequenzy Ablation Cryosurgery Local Chemotherapy Percutaneous Ethanol Injection Systemic Chemotherapy
Liver Cancer Treatment Percutaneous Ethanol Injection (PEI) PEI is a local tumour ablative technique depending on the toxic effects of ethanol (alcohol) Ethanol causes • Protein denaturation • Cellular dehydration
Liver Cancer Treatment Percutaneous Ethanol Injection (PEI) Procedure: Most common is the ‘Multi-Session’ approach in an outpatient setting In each session 8-10ml ethanol are injected in the tumour under local anesthesia and ultrasound guidance. Complications are systemic alcohol intoxication, transient pain and fever
Liver Cancer Treatment Percutaneous Ethanol Injection (PEI) Outcome: There are only data for HCC available, these only retrieved from retrospective reviews without control. HCC 1 year survival 93% 2 year survival 80% 3 year survival 68%
Liver Cancer Treatment Surgical Resection Liver Transplantation Radiation Therapy Radiofrequenzy Ablation Cryosurgery Local Chemotherapy Percutaneous Ethanol Injection Systemic Chemotherapy
Liver Cancer Treatment Systemic Chemotherapy Systemic chemotherapy is not regarded as an effective treatment, neither in HCC nor in metastatic liver cancer Liver cancers have been found to be relatively resistant to chemotherapeutic drugs at systemic doses and the reported response rate is less than 30% The chemotherapy regimen in secondary liver cancer is therefore determined by the type of the primary cancer and only palliative with regard to the liver.