Download
1 / 42
430 likes | 572 Views
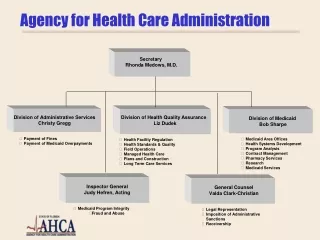
HCAD 5387 Information Systems for Health Care Administration. Session 1: Health Information http://thecolbertreport.cc.com/videos/udr4lu/eric-topol. Introduction.

E N D
HCAD 5387Information Systems for Health Care Administration Session 1: Health Information http://thecolbertreport.cc.com/videos/udr4lu/eric-topol
Introduction • One of the most common themes in just about every current or recent past plan to reform healthcare has been the reliance on IT to deliver • Lower Costs • Fewer errors • Better outcomes • Increased overall system efficiencies
Creative Destruction of Medicine New Medicine Creative Destruction Mobile Connectivity + Bandwidth Wireless Censors Super Convergence Genomics Internet Imaging Social Networking Information Systems Computing Power + Data Universe Old Medicine
Introduction • One of the main expected drivers is electronic medical records • But that is not the only area • Improved information on diagnosis • Coordination • Delivery • From Population to Individual Medicine
American College of Physicians and AmericanEHRPartners:“Challenges with Meaningful Use: EHR Satisfaction & Usability Diminishing” Satisfaction and usability ratings for certified electronic health records have decreased since 2010. Overall, user satisfaction fell 12 percent from 2010 to 2013. The percentage of clinicians who would not recommend their EHR to a colleague increased from 24 percent in 2010 to 39 percent in 2013. Clinicians who were "very satisfied" with the ability for their EHR to improve care dropped by 6 percent compared to 2010, while those who were "very dissatisfied" increased by 10 percent. Thirty-four percent of users were "very dissatisfied" with the ability of their EHR to decrease workload — an increase from 19 percent in 2010. In 2013, 32 percent of the responders had not returned to normal productivity compared to 20 percent in 2010. Dissatisfaction with ease-of-use increased from 23 percent in 2010 to 37 percent in 2013, while satisfaction with ease-of-use dropped from 61 to 48 percent
National Bureau of Economic ResearchHospital-Level IT adoption “Health IT and Patient Outcomes” (health economists at Minnesota/PENN) Health IT adoption reduces mortality for the most complex patients but does not affect outcomes for the median patient. Benefits from IT adoption are skewed to large institutions with a severe case mix Benefits are primarily experienced by patients whose diagnoses require cross-specialty care coordination
Introduction • We have a long way to go • About 40% of physicians and 27% of hospitals are using basic electronic health records • But we’ve made progress – just 4 years ago these percentages were 20% and 10%, respectively • However, relatively few are meaningfully applying health IT to advance care coordination, aide clinical decision making, or report health outcomes. • So there is potential but no guarantees
Introduction Ask Heath care executives if they feel good about the quality, accessibility, and timeliness of clinical and business data at their organization and the answer is generally – NO Why? Or why is healthcare so far behind?
Why does Healthcare Lag in IT? • Large number of small organizations • Incentives are misaligned • Better management of chronically ill may actually cost providers money. • Goals of physicians may be different from goals of hospital • Higher quality/more efficient care may not result in increased “customers” • Fragmented system • Network externality • Complexity of care • Health care vs. Banking • What is happening to try to resolve this?
HITECH • Health Information Technology for Economic and Clinical Health – HITECH • Part of the 2009 American Recovery and Reinvestment Act • In February 2010 $750 million in grants and contracts went to agencies in 40 states and to 30 nonprofit organizations to “facilitate the exchange of health information.” • Also $225 million to 55 training programs to help train people for jobs in the health care and Health IT sectors.
HITECH • Carrots and Sticks • The carrots: • $14-27 billion will go to physicians, hospitals and other providers in the form of bonuses on their Medicare and Medicaid payments. • Fiscal year 2011 (October 2010) to hospitals • January 2011 physicians (up to $18,000) • If they can demonstrate that they are making “meaningful use” of health IT in addition to merely purchasing it and installing it. • Then comes the stick • In 2015(6?) payments will be replaced by penalties for those not showing meaningful use.
HITECH • Responsibility for implementing provisions held by HHS Office of the National Coordinator for Health IT • Dr. Karen B. DeSalvo, MD, MPH, MSc • Formerly FarzadMostashari, David Blumenthal • August 2010 plan for certifying electronic health record systems was released. • Functional • Interoperable • Secure
Defining Meaningful Use http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Stage_2.html
What is MU? • To receive an EHR incentive payment, providers have to show that they are “meaningfully using” their EHRs. • Stage 1 • 13 (hospitals) or 14 (professionals) core objectives that must be met • 5 objectives from a menu of 10 • Focus is on having technology in place and collecting data • Stage 2 – 2014 for those who started in 2011 • Similar criteria must be met • But focus is on using the data • Stage 3 • Focus on achieving improvements in quality, safety, and efficiency
1. Introduction • But what exactly is “IT”? • The book breaks the subject into 4 basic areas • Healthcare information • Define health information • Data quality • Regulations, Laws, and Standards of Health Information • Healthcare Information Systems • Evolution of Health Systems – past and future • Selection and Implementation
1. Introduction • Information Technology • The core technology behind the systems – how they work • Architectures • Databases, networks, standards, and security • The idea is not to make you great programmers, but to be able “speak the language” a little better • Top Level View of IT • How IT departments are organized • IT’s role in strategy • Budgeting and governance • Managing Change
Chapter 1: Health Care Information • What is Healthcare Information? • HIPAA, Protected Health Information (PHI): Any information, whether oral or recorded in any form or medium that • Is created or received by a health care provider, health plan, public health authority, employer, life insurer, school or university, or health care clearinghouse, and • Relates to the past, present, or future physical or mental health or condition of an individual, the provision of health care to an individual, or the past, present, or future payment for the provision of health to an individual
Information • National Alliance for Health Information Technology Definitions • Electronic Medical Record: An electronic record of health related information on an individual that can be created, gathered, managed, and consulted within one organization • Electronic Health Record: conforms to nationally recognized interoperability standards, across more than one organization • Personal Health Record: conforms to nationally recognized interoperability standards, drawn from multiple sources, managed shared, and controlled by the individual.
Joint Commission and Information • Patient-Specific data and information (LOS) • Aggregate data and information (ALOS) • Comparative data and information • Combining internal and external data to aid organizations in evaluating their performance • Knowledge-based information • a collection of stored facts, models and information that can be used for designing and redesigning processes and for problem solving. It is found in the clinical, scientific and management literature
Purpose of Patient Records Patient Care Communication Legal Documentation Billing and Reimbursement Research and Quality Management
Content of Patient Records Identification Problem list Medication record (MAR) History and physical Progress notes Consultation Physician’s orders Imaging and x-ray reports Laboratory reports Consent and authorization forms Operative report Pathology report Discharge summary
Administrative Data • One of the primary purposes on the administrative data side is billing. • A big part of all this deals with diagnosis and procedure codes. • CPT-4 Current Procedural Terminology -- the standard for physician’s office, outpatient, and ambulatory care coding for reimbursement purposes. • ICD-9-CM International Classification of Diseases, Ninth Revision, Clinical Modification • Hospitals use this to determine which DRG the patient falls in
Move to ICD-10 • Starting on October 1 20132014 2015 ICD-10 will replace ICD-9 • Originally planned to adopt earlier, but significant push back by providers • Belief is that ICD-9 is outdated and new codes will provide more specificity and better data for public health surveillance and research initiatives. • This will be a huge deal in terms of impact and cost. • Lots of practice management and other electronic systems cannot accommodate the ICD-10 codes and need to be replaced
Move to ICD-10 • ICD-10-CM codes used in documenting diagnoses (cm=clinical modification) • 3-7 characters in length and total 68,000 • ICD-9-CM are 3-5 digits and number over 14,000 • ICD-10-PCS are the procedure codes and are alphanumeric • 7 characters in length and total about 87,000 procedures • ICD-9-PCS procedure codes are only 3-4 numbers in length and total about 4,000 codes
Specificity looks like this… ICD-9-CM 821.01 Fracture of femur, shaft, closed ICD-10-CM Many possible codes
Benefits Codes in ICD-10 are more specific, which means… • Improved care management of beneficiaries • Clinical data with greater specificity • Reliable and robust clinical data that can be used to make intelligent, data driven decisions • More accurate payments • Reduced number of miscoded, rejected and improper reimbursement claims • Better data for fraud and abuse monitoring
Benefits Cont’d Better understanding of the value of new medical procedures Improved disease management Better understanding of healthcare outcomes More ICD codes to address global disease emergencies
Challenges of Implementation Training Converting Systems & Interfaces Ensuring readiness across vendors and payers Payer contracts Potential slow-down in dropping claims Documentation Improvement Rewriting reports & queries Budget
Financial Impact • $30 Billion – U.S. • a 10-physician practice $285,000 (MGMA) • Smaller practices is about $83,000 (MGMA) • $2-3 Million – for a typical large hospital system • Testing • Training • Productivity Losses • Revenue Losses • Reimbursement • System Changes
AMA and ICD 9 10 11? • The AMA policy has been “vigorously working to stop the implementation of the ICD-10” • For over a decade they have persuaded CMS to hold off under the argument that it is too burdensome on physicians • Currently we are set to adopt ICD-10 October 15. • The World Health Organization is set to consider ICD-11 in May of 2015 • There was some push to skip straight from ICD-9 to ICD-11 • But the AMA just issued a report arguing against going to 11 • Basically ICD-9 is outdated and it limits the ability to correctly code • It will be hard enough to get to ICD-10, ICD-11 will be a disaster
Chapter 2: Health Care Quality Data • This chapter stresses the importance of quality when it comes to data • Data vs. Information • Information is processed data • Data are raw facts, not very useful for decision making. • One of the keys to turning data to information is having quality data
Problems of Poor Quality Data • Diminished quality of Patient care data can lead to problems with • Patient care • Communication among providers & patients • Documentation • Reimbursement • Outcomes assessment • Research
American Health Information Management Association(AHIMA) Data Quality Model • Accuracy • Accessibility • needs to be available to the appropriate decision maker • Comprehensiveness • Consistency • e.g., abbreviations • Currency • diagnosis on discharge can be different than on admission. • if you want a report on the diagnoses treated during a particular time frame, which of these two diagnoses should be included? • Definition • easy to understand definitions, data dictionaries • how many people are in this class?
American Health Information Management Association(AHIMA) Data Quality Model • Granularity – or atomicity. • Data elements are “atomic” in the sense that they cannot be further subdivided. • Eg, a patient’s name is stored as three elements: last, first, middle. Not as one element. • Census – daily for staffing, monthly for long range planning. • Precision – how close to actual size, weight, or other standard does the data need to be? Drug dose, LOS • The necessary precision in recording outdoor temp is different from recording patient temp (100 vs. 99.6o) • Relevancy – the question or aim of the data must be clarified to ensure relevant data • Timeliness – HCAHP Scores
Types and Causes of errors • Systematic vs. random errors • Systematic errors are those that can be attributed to standard procedures (the procedure is broken) • Random errors are not attributed to a flaw in the system • IT can help with many of these errors
Using IT to Improve Data Quality • Data Error Prevention • Compose a minimum set of necessary data items • Define data and data characteristics in a data dictionary • Develop a data collection protocol • Create user friendly data entry forms or interface • Compose data checks • Create a quality assurance plan • Train and motivate users
Using IT to Improve Data Quality • Data Error Detection • Perform automatic data checks • Perform data quality audits • Review data collection protocols and procedures • Check inter- and intraobserver variability • Visually inspect completed forms • Routinely check completeness of data entry
Using IT to Improve Data Quality • Actions for Data Quality Improvement • Provide data quality reports to users • Correct inaccurate data and fill in incomplete data detected • Control user correction of data errors • Give feedback of data quality results and recommendations • Resolve identified causes of data errors • Implement identified system changes • Communicate with users