Download
1 / 23
280 likes | 652 Views
Management of Colorectal Liver Metastasis. Joint Hospital Grand Round Dr. Edgar Lau Department of Surgery, PYNEH 12/1/2008. Background. Liver metastasis is most frequently seen in patient with colorectal carcinoma 15-25% present at the time of diagnosis

E N D
Management of Colorectal Liver Metastasis Joint Hospital Grand Round Dr. Edgar Lau Department of Surgery, PYNEH 12/1/2008
Background • Liver metastasis is most frequently seen in patient with colorectal carcinoma • 15-25% present at the time of diagnosis • Additional 20-25% develop metachronous hepatic tumors • In 30%, liver is the only site of metastatic disease
Background • Carries a dismal prognosis without intervention • 5-year survival 0-2% • Median survival 6-12 months
Treatment Modalities • Surgery • Local Ablative Therapy • Radiofrequency ablation • Chemotherapy
Surgery • Hepatic resection remains the only hope for cure in metastatic colorectal carcinoma • Large series from 1960s through mid-1990s reported 5-year survival rates around 33-36%
Prognostic Factors • Stage, grade, nodal status of primary colorectal tumor • Disease-free interval • Number and distribution of liver metastases • Pre-operative CEA level • Extrahepatic disease • Fong Y et al: Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: Analysis of 1001 consecutive cases. Ann Surg 1999 • Positive nodal status • Multiple tumors • Disease-free interval < 12 months • CEA level > 200 ng/mL • Tumor size > 5 cm
Reasons for Improvement • Better patient selection • Improved anesthetic monitoring • Greater understanding of hepatic anatomy • Advances in surgical technique • Improved perioperative critical care • More effective adjuvant therapy
Resectability • Macroscopic and microscopic (R0) treatment of the disease is feasible with either resection alone or resection combined with RFA • Two adjacent liver segments can be spared • Vascular inflow, outflow, and biliary drainage can be preserved • Sufficient remnant liver volume (> 20% of total estimated liver volume)
Extent of Surgical Margin • Multiple studies have shown that clear margins are essential for long-term outcomes • Extent of margin is controversial • earlier series reported at least 1 cm • recent series have shown that survival is not associated with width of negative margin
Two-stage Hepatectomy • For patients with multiple hepatic colorectal metastasis who are not candidates for a complete resection by single hepatectomy • even after portal vein embolization (PVE) or downsizing by chemotherapy • Adam R et al: Two-stage hepatectomy: A planned strategy to treat irresectable liver tumors. Annals of Surgery, 2000 • 16 patients • post-op complication higher in second stage • 3-year survival = 35%; Median survival 44 months from diagnosis
Two-stage Hepatectomy • Done with curative intent • Future functional liver remnant resected in first stage • followed by PVE to contralateral side and allow remnant hypertrophy
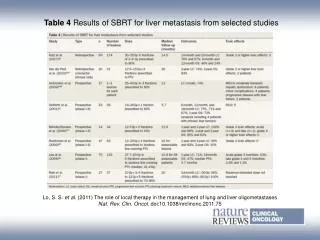
Radiofrequency Ablation • To treat tumors which do not meet resectability criteria, but disease confined to the liver or stable extra-hepatic disease • Not as a replacement for resection • Expand the number of surgical candidates • Solbiati L et al. Percutaneous radiofrequency ablation of hepatic metastases from colorectal cancer: long-term results in 117 patients. Radiology, 2001 • 117 patients • 3-year survival 46% • median survival 36 months • Only 6 studies that reported at least 3-year survival were identified, with results ranging from 37-58% • McKay et al: Current role of radiofrequency ablation for the treatment of colorectal liver metastases. BJS, 2006
RFA + Surgery • Abdalla EK et al. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal metastases. Ann Surg, 2004
RFA + Surgery • Recurrence • RFA 84% • RFA + resection 64% • Resection 52% • 4 year survivial • RFA 22% • RFA + resection 36% • Resection 65%
Neoadjuvant Chemotherapy • Enable downstaging of unresectable tumors to potentially resectable • Masi G et al: Treatment with 5-FU/folinic acid, oxaliplatin and irinotecan enables surgical resection of metastases in patients with initially unresectable metastastic colorectal cancer. Ann Surg Oncol. 2006 • 74 patients • 26% were able to undergo surgery • median survival 36.8 months (vs. 22.2 months)
Adjuvant Chemotherapy • Role of adjuvant chemotherapy after potentially curative resection is ill-defined • High percentage of patients with resection develop recurrence • undetectable disease likely present at time of surgery
Advantages Allows time for other metastastic sites to become clinically evident Allows for in vivo gauge of chemoresponsiveness, facilitating post-operative chemotherapy planning Response may allow for easier resection and increased rate of negative surgical margins Response may be a prognostic factor Disadvantages Tumor may progress to unresectable status Perioperative morbidity may be increased because of hepatotoxicity of chemotherapy Possible loss to surgical follow-up Patient anxiety and desire to have tumor resected as soon as possible Pre-op vs. Post-op Chemotherapy
Chemotherapy for Palliation • Traditional therapy include fluorouracil in addition to leucovorin • response rate from 20-30% • median survival 11.5 months • Irinotecan • higher response rate when added to traditional 5-FU/leucovorin and longer overall survival (14.8 months) • Oxaliplatin • less toxic compared to irinotecan/5-FU/leucorvorin
Synchronous Hepatic Metastasis • Noted in 15-20% of patients • Synchronous or delayed (8-12 weeks) • Optimal timing is not well defined • Recent studies have shown comparable hospital stay, morbidity and perioperative mortality • Martin R et al: Simultaneous liver and colorectal resections are safe for synchrous colorectal liver metastasis. J Am Coll Surg, 2003 • Chua HK et al: Concurrent vs. staged colectomy + hepatectomy for primary colorectal cancer with synchrous hepatic metastasis. Dis Colon Rectum, 2004 • Synchronous therapy allows earlier completion of all phases of therapy +/- adjuvant therapy initiation • Decision should be individualized based on complexity of surgery
Recurrence • 50-60% develop recurrent liver metastasis after resection • Approximately 20-30% potentially amendable to further resection with isolated intrahepatic disease • 5-year survival rates ranging from 16-41% • Same criteria as for initial hepatectomy
Take Home Message • Surgery remains the only reliable long-term cure • Increasing number of modalities to tackle patients who are deemed “unresectable” • Treatment modalities should be tailored according to individual patients