Download
1 / 78
840 likes | 1.28k Views
Anesthesia at the Extremes of Altitude and Environment. Major Eric Weissend, M.D. Department of Anesthesiology Wilford Hall Medical Center Lackland AFB, Texas. Environmental Challenges in the Practice of Anesthesiology.

E N D
Anesthesia at the Extremes of Altitude and Environment Major Eric Weissend, M.D. Department of Anesthesiology Wilford Hall Medical Center Lackland AFB, Texas
Environmental Challenges in the Practice of Anesthesiology • Air Force anesthesiology providers are now going far and wide in support of combat and humanitarian operations. The majority of postings are to minimally developed areas where patients and providers are subject to environmental extremes.
Environmental Challenges in the Practice of Anesthesiology • Deployment presents numerous personal and professional challenges. Caring for trauma and surgical disease in the deployed environment can be physically and intellectually challenging. The extremes of heat, cold, and altitude further complicate the care of our patients.
Environmental Challenges in the Practice of Anesthesiology • Military operations in Afghanistan and Iraq serve to illustrate theses types of environments.
Heat • Iraq: Daytime temperatures in the summer regularly reaching well over 100 degrees F.
Cold • Afghanistan, Operation Anaconda: Soldiers fought for extended periods in temperatures well below freezing in the mountainous Shah-I-Khot region.
Altitude • Afghanistan, Operation Anaconda (again): Combat Ops took place between 8,000 and 12,000 feet above sea level. • Bagram Air Base located at 5,000 feet above sea level.
Environmental Challenges in the Practice of Anesthesiology • To provide safe and effective anesthesia services to our patients we must understand the effects that extremes of heat, cold, and altitude have on our patients, ourselves, and our equipment.
How Does Excessive Ambient Heat Effect Anesthetic Practice? • Effects on volatile anesthetics • Heat injuries
Inhaled Anesthesia and Heat • Temperature effects vaporizer output minimally in normal ranges of temperatures. • All vaporizers in use in the EMEDS and MFST systems are temperature compensated. • In a consistently climate controlled environment altered output should not be an issue.
Inhaled Anesthesia and Heat • Narkomed M: Currently the Air Force standard anesthesia machine for field anesthesia operations. This machine is equipped with the Draeger Vapor 2000 anesthetic vaporizer. • Draeger Vapor 2000 vaporizer is temperature compensated with an operating range of 10 to 40 degrees C (50-104 degrees F)
Ohmeda Portable Anesthesia Circuit (PAC) with Draw-over Vaporizer
Inhaled Anesthesia and Heat • The Ohmeda Portable Anesthesia Circuit (PAC) Draw-Over Vaporizer System (primarily still in use with MFST). • Operating temperature for the PAC vaporizer is 18 to 35 degrees C (65-95 degrees F).
Inhaled Anesthesia and Heat • Use above this ambient temperature range may lead to “potentially hazardous excessive concentrations of anesthetic agent.”
Inhaled Anesthesia and Heat • “Under no circumstances must the temperature of the anesthetic agent reach boiling point, as the output concentration will then become impossible to control.” • The boiling points for isoflurane, halothane, and sevoflurane are 48.5, 50.2, and 58.5 degrees C (119, 122.4, 137 degrees F) respectively at 760 mm Hg.
Inhaled Anesthesia and Heat • Is it conceivable that in Iraq, in July, the HV/AC system may fail intraoperatively?
If using volatile anesthetics at high ambient temperatures • Ensure you are operating in a consistent climate controlled environment. AND/OR • Use only with end tidal anesthetic gas monitoring (RGM or other) to minimize the risk of volatile anesthetic overdose.
Inhaled Anesthesia and Heat • There currently is no means of monitoring inspiratory or expiratory anesthetic gas in any Air Force deployable anesthetic system.
Other Anesthetic Options at High Ambient Temperatures • Total Intravenous Anesthesia • Regional Anesthesia Neither method is known to be effected by high ambient temperatures.
Heat Injuries • Heat illness is the inability of normal regulatory mechanisms to cope with a heat stress • Minor injuries include muscle cramps, edema, rash, syncope, and tetany • Major injuries are heat exhaustion and heat stroke • All heat injuries are manifestations of dehydration
Heat Injuries • Patients who are injured in and evacuated from areas with high ambient temperatures may suffer heat injuries in addition to their traumatic wounds. • Medical personnel suffering heat injuries may have difficulty or even be unable to care for their patients.
Heat Injuries • Any condition that increases heat gain or decreases heat loss may result in a major heat illness. • Hot environments and physical exertion increase the heat load. • Strenuous exertion can increase endogeonous heat production ten to twenty-fold. • High temperatures and high humidity inhibit heat loss.
Heat Injuries Photo by Wally Santana/The Associated Press
Heat Injuries • Peripheral vasodilation and sweating are the primary mechanisms of heat loss • Evaporation of sweat from the skin is the most important mechanism of heat dissipation. • As humidity increases, the efficiency of sweating decreases.
Heat InjuriesHeat Exhaustion • Caused by dehydration with inadequate fluid and electrolyte replacement. • Usually in nonacclimatized persons who have been working in the heat for several days.
Heat InjuriesHeat Exhaustion • Symptoms Weakness, fatigue, frontal headache, impaired judgement, vertigo, nausea and vomiting, muscle cramps Orthostatic dizziness and syncope Sweating persists, often profuse Core temperature less than 40 C No signs of severe CNS damage
Heat InjuriesHeat Exhaustion • Volume depletion is the primary problem • Treatment Rest in cool environment Fluid resuscitation
Heat InjuriesHeat Stroke • A catastrophic life threatening medical emergency • The failure of normal homeostatic cooling mechanisms • Leads to extremely high temperatures (>40.5C), multisystem tissue damage and organ dysfunction.
Heat InjuriesHeat Stroke • Symptoms • Profound CNS dysfunction is the Hallmark Delerium and coma are common Any neurologic manifestation is possible • Dry hot skin, though sweating can persist • Cardiovascularly hyperdynamic • Hepatic dysfunction with massive rise in transaminases • Coagulopathy • Renal damage with acute renal failure in up to 30% of cases.
Heat InjuriesHeat Stroke • Treatment • Core Temperature Cooling Evaporative cooling with fans and skin wetting Ice-water immersion Ice packs, cooling blankets, cool body cavity lavages • Supportive Therapy Airway management (aspiration and seizures are common) Resuscitation and invasive monitoring
Anesthesia At Altitude • As altitude increases atmospheric pressure decreases. • Decreased atmospheric pressure has profound effects on inhaled anesthetics and human physiology. • Safe and effective anesthesia care requires an understanding of all of these effects.
Anesthesia At Altitude • The composition of the atmosphere is fixed and is independent of altitude. Oxygen is always ~21% of the ambient atmosphere pressure. • As atmospheric pressure decreases with elevation however, the partial pressure of oxygen (PO2) declines.
Anesthesia At Altitude • Recall the alveolar gas equation: PAO2=FiO2(PB-PH2O)-PaCO2/RQ At 5000ft elevation, PB is 632 mmHg, PaO2 is 81 mmHg with SaO2 95%. At 10,000ft elevation, PB is 522 mmHg, PAO2 is 59 mmHg, SaO2 84%.
Oxygen-Hemoglobin Dissociation Curve. Approximate oxygen saturations are marked for several altitudes Sutton JR, et al: J Appl Physiol 64:1309, 1998
Anesthesia At Altitude • “In addition, it is important to maintain a higher concentration of oxygen both during and after administration of the anesthetic to support adequate oxygenation. It is suggested that 30% oxygen be the minimum at 5000 ft and that 40% oxygen be the minimum at 10,000 feet, for both intraoperative anesthetic management and postoperative recovery.”
Anesthesia At Altitude • Recommendations for anesthesia at altitude: “The major risk of anesthesia at high altitude is that anesthetized patients can become hypoxic despite the fact that adequate oxygen concentrations are being administered.”
Anesthesia At Altitude • Nitrous Oxide • Essentially irrelevant. Unlikely to be available in the deployed environment. Efficacy of N2O is decreased by 50% at 5000 ft and essentially insignificant at 10,000 ft.
Anesthesia At Altitude • Volatile anesthetic agents • “The saturated vapor pressure of a volatile anesthetic agent depends only on temperature and is practically independent of total environmental pressure”
Anesthesia At Altitude • Given the relative scarcity of gaseous (or liquid) oxygen in the deployed environment it may be reasonable to conduct as much anesthesia under regional techniques. • At altitude, maximizing the use of regional anesthesia not only decreases use of scarce resources, but may improve patient safety postoperatively. Minimizing opioid use decreases the risk of postoperative respiratory depression.
Anesthesia At Altitude • If general anesthesia is required oxygen requirements may be minimized using TIVA techniques.
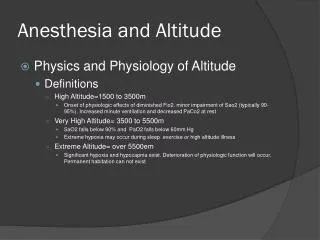
Altitude Illness • Military personnel deployed rapidly to high altitude regions are all at risk for altitude related illnesses. • High altitude begins at 1500m (~5000ft) above sea level. • Very high altitude begins at 3500m (~11,500 ft) • Extreme altitude begins at 5500m (~18,000 ft)
Altitude Illness • Physiologic adjustment to altitude requires time and patience. • Sudden exposure to very high and extreme altitude (above 11,500 ft) can be fatal. • Unconciousness can occur within minutes and death may follow without supplemental oxygen.
Physiologic Response to Altitude • Lower PB leads to lower PAO2, decreased SAO2 and PaO2 and elevated Alveolar-arterial oxygen gradients. • Hypoxic Ventilatory Response to low PaO2 leads to hyperventilation. • Hyperventilation leads to decreased PaCO2.
Physiologic Response to Altitude • As hyperventilation is the primary means of adaptation to ascent, the ability to tolerate hypoxic environments depends largely on sufficient pulmonary reserve.
Physiologic Response to Altitude • 2,3-DPG levels rise due to hypoxic stress, shifting O2-Hgb dissociation curve back toward the right. This facilitates O2 unloading into tissues. • Erythropoiesis • Increased cardiac output secondary to Hypoxia
Altitude Illness • High Altitude Illness can take several forms that often overlap and share common pathophysiology. • Acute Mountain Sickness (AMS) • High Altitude Pulmonary Edema (HAPE) • High Altitude Cerebral Edema (HACE)
Acute Mountain Sickness • All visitors to higher altitudes are susceptible to AMS. • Overexertion, poor hydration, and young age may contribute. Physical fitness and gender don’t seem to effect incidence.
Acute Mountain Sickness • Symptoms: • Early symptoms (12-24 hours): headache refractory to standard analgesics, nausea, anorexia, lassitude, sleep disturbances. • Can progress to shortness of breath, intense snoring, vomiting, hallucinations, and impaired cognitive function, • Advanced symptoms: severe dyspnea, cyanosis, decreased SaO2, ataxia.