
Impact of Opioid Use Changes on Chronic Low Back Pain: One-Year Study Results
Investigating the correlation between changes in opioid use and health outcomes in chronic low back pain patients over a one-year period. Findings show improved health outcomes but no significant correlation with opioid use changes. Results suggest age and comorbidities may influence opioid initiation. Funding: Residency Research Network of Texas, Dean’s Office, School of Medicine, UTHSCSA.

Impact of Opioid Use Changes on Chronic Low Back Pain: One-Year Study Results
E N D
Presentation Transcript
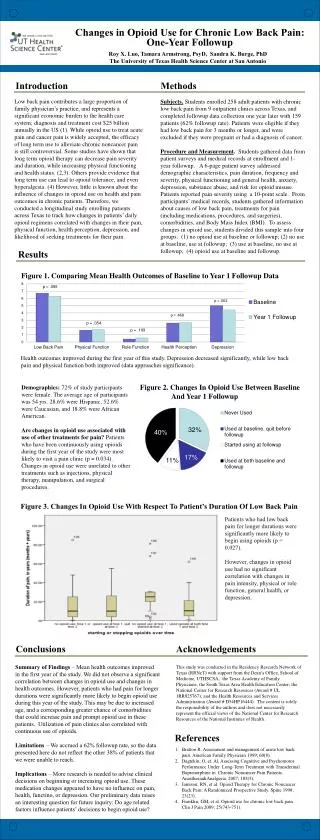
Changes in Opioid Use for Chronic Low Back Pain: One-Year Followup Roy X. Luo, Tamara Armstrong, PsyD, Sandra K. Burge, PhD The University of Texas Health Science Center at San Antonio Introduction Methods Low back pain contributes a large proportion of family physician’s practice, and represents a significant economic burden to the health care system; diagnosis and treatment cost $25 billion annually in the US (1). While opioid use to treat acute pain and cancer pain is widely accepted, the efficacy of long term use to alleviate chronic noncancer pain is still controversial. Some studies have shown that long term opioid therapy can decrease pain severity and duration, while increasing physical functioning and health status. (2,3). Others provide evidence that long term use can lead to opioid tolerance, and even hyperalgesia. (4) However, little is known about the influence of changes in opioid use on health and pain outcomes in chronic patients. Therefore, we conducted a longitudinal study enrolling patients across Texas to track how changes in patients’ daily opioid regimens correlated with changes in their pain, physical function, health perception, depression, and likelihood of seeking treatments for their pain. Subjects. Students enrolled 258 adult patients with chronic low back pain from 9 outpatient clinics across Texas, and completed followup data collection one year later with 159 patients (62% followup rate). Patients were eligible if they had low back pain for 3 months or longer, and were excluded if they were pregnant or had a diagnosis of cancer. Procedure and Measurement. Students gathered data from patient surveys and medical records at enrollment and 1-year followup. A 6-page patient survey addressed demographic characteristics, pain duration, frequency and severity, physical functioning and general health, anxiety, depression, substance abuse, and risk for opioid misuse. Patients reported pain severity using a 10-point scale. From participants’ medical records, students gathered information about causes of low back pain, treatments for pain (including medications, procedures, and surgeries), comorbidities, and Body Mass Index (BMI). To assess changes in opioid use, students divided this sample into four groups: (1) no opioid use at baseline or followup; (2) no use at baseline, use at followup; (3) use at baseline, no use at followup; (4) opioid use at baseline and followup. Figure 2. Changes In Opioid Use Between Baseline And Year 1 Followup Results Figure 3. Changes In Opioid Use With Respect To Patient’s Duration Of Low Back Pain Figure 1. Comparing Mean Health Outcomes of Baseline to Year 1 Followup Data Patients who had low back pain for longer durations were significantly more likely to begin using opioids (p = 0.027). However, changes in opioiduse had no significant correlation with changes in pain intensity, physicalor role function, general health, or depression. Health outcomes improved during the first year of this study. Depression decreased significantly, while low back pain and physical function both improved (data approaches significance). Demographics: 72% of study participants were female. The average age of participants was 54 yrs. 28.6% were Hispanic, 52.6% were Caucasian, and 18.8% were African American. Are changes in opioid use associated with use of other treatments for pain? Patients who have been continuously using opioids during the first year of the study were most likely to visit a pain clinic (p = 0.034). Changes in opioid use were unrelated to other treatments such as injections, physical therapy, manipulation, and surgical procedures. Conclusions Acknowledgements This study was conducted in the Residency Research Network of Texas (RRNeT) with support from the Dean’s Office, School of Medicine, UTHSCSA; the Texas Academy of Family Physicians; the South Texas Area Health Education Center; the National Center for Research Resources (Award # UL 1RR025767); and the Health Resources and Services Administration (Award # D54HP16444). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources of the National Institutes of Health. Summary of Findings – Mean health outcomes improved in the first year of the study. We did not observe a significant correlation between changes in opioid use and changes in health outcomes. However, patients who had pain for longer durations were significantly more likely to begin opioid use during this year of the study. This may be due to increased age, and a corresponding greater chance of comorbidities that could increase pain and prompt opioid use in these patients. Utilization of pain clinics also correlated with continuous use of opioids. Limitations – We accrued a 62% followup rate, so the data presented here do not reflect the other 38% of patients that we were unable to reach. Implications – More research is needed to advise clinical decisions on beginning or increasing opioid use. These medication changes appeared to have no influence on pain, health, functino, or depression. Our preliminary data raises an interesting question for future inquiry: Do age related factors influence patients’ decisions to begin opioid use? References • Bratton R. Assessment and management of acute low back pain. American Family Physician 1999; 60(8). • Dagtekin, O, et. Al. Assessing Cognitive and Psychomotor Performance Under Long-Term Treatment with TransdermalBuprenorphine in Chronic Noncancer Pain Patients. Anasthesia&Analgesia. 2007; 105(5). • Jamison, RN, et al. Opioid Therapy for Chronic Noncancer Back Pain: A Randomized Prospective Study. Spine 1998; 23(23). • Franklin, GM, et al. Opioid use for chronic low back pain. Clin J Pain 2009; 25(743-751).





