Download
1 / 52
520 likes | 617 Views
Chapter 26. Urinary System. Urinary System Functions. Filtering of blood Regulation of blood volume concentration of blood solutes pH of extracellular fluid blood cell synthesis Synthesis of Vitamin D Increased PTH promotes Vitamin D formation in the kidneys. 1. Overview

E N D
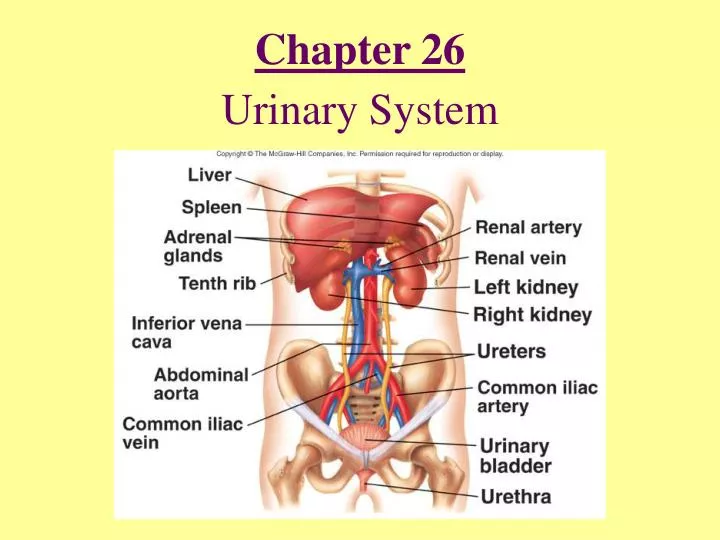
Chapter 26 Urinary System
Urinary System Functions • Filtering of blood • Regulation of • blood volume • concentration of blood solutes • pH of extracellular fluid • blood cell synthesis • Synthesis of Vitamin D Increased PTH promotes Vitamin D formation in the kidneys
1. Overview The urinary system is the system responsible for removing organic wastes from the body in a liquid form. By doing so in an appropriate manner, the urinary system contributes to the homeostasis of the body. They regulate:Blood volume, blood pressure, plasma electrolytes, pH, blood glucose and, blood amino acids, etc. It is also important to note how the urinary system is isolated from the circulatory system to avoid contamination.
The manner how the urinary system works is unique. It first filters out water, electrolytes and small organic molecules into the capsular space, then one by one reabsorb those which are needed back from the tubules and ducts. If the urinary system fails to properly filter and reabsorb these vital ions and molecules, they may be wasted into the urine. Thus, by observing what you find in the urine you may be able to judge the health of a subject. An adult produces about 1.4 L of urine per day. Note each adult consume about 2L of liquid each day. Where did the rest go?
Internal Anatomy of Kidneys • Cortex: Outer area • Renal columns • Medulla: Inner area • Renal pyramids • Calyces • Major: Converge to form pelvis • Minor: Papillae extend • Nephron:Functional unit of kidney • Juxtamedullary • Cortical
i. Overall Functions of the nephron • The basic functional units of the kidney are shown in Fig. 26-6. • The formation of urine starts with the filtrates from arterial blood, which will be released into the renal corpuscle. • In the renal corpuscle, blood pressure in the renal arterioles pushes water, electrolytes and small organic molecules into the capsular space ( Bowman’s space) across the glomerular walls. • Small important substance, which have passed through the pores of the membrane must be reclaimed, while keeping the wastes in the collecting duct..
i. The blood supply to the kidneys • 1200 ml/min through the kidneys • Consumes 20 - 25% of the cardiac output! • Study Fig. 26-7b,2 and Fig. 26.6 of Seeley, and follow the direction of blood vessels. • Note the afferent and efferent arterioles. • Where are the peritubular capillaries • What are vasa recta?
a. The basic principles of urine production • The reason for urine production is to maintain the homeostasis of the blood. • The urine collects metabolic waste products.
i. There are three major waste products in urine: Table 26-2 • (a) Urea form the breakdown of amino acids. 21 g/day. • (b) Creatinine from the breakdown of creatine phosphate, recall muscle contraction. 1.8 g/day. • (c ) Uric acid from RNA. 0.48 g/day. • These wastes filter through glomerular membranes with a large quantity of water and ions. In other words, the concentrations of these ions and molecules in the in the filtrate and plasma are the same.
i. The majority of water must be reclaimed to avoid dehydration. • Water is first filtered through the pores of glomerular membrane by the blood pressure into the Bowman’s space. • Resorption for reclaiming water, electrolytes, small organic molecules either by simple diffusion or with the carrier proteins at the proximal tubule starts immediately. Fig. 26.8 of SeeleyResorption of water continues at the descending limb of the loop of Henle. Fig. 26-13b
Filtration at the glomerulus • (a) The glomerular filtration pressure (Fig. 26-8, 10, Fig. 26.9) • The driving force at the glomerular is the difference between the blood pressure and osmotic pressure. • The net filtration pressure is about 7 mmHg and is very small. • Thus, slight change in blood pressure could change the magnitude of this driving force and can impair the function of the kidneys. • Note that the muscles of arterioles can easily change the diameters, thus the regional blood pressure.
(a) The glomerular filtration rate (GFR) • The filtration surface area of each kidney is 6 sq m. • GFR is 125 ml/min for each kidney or 250 ml/min for the both kidneys. • Since a 1,200 ml/min of blood is supplied to the kidneys, and about a half of it are fluid, more than 40% of fluid in the blood are filtered. • 360 liters (100 gallons) are filtered through per day. • But 99% of the filtrates are reabsorbed. • The GFR may be regulated with hormone.
(a) The proximal (convoluted) tubule (PCT) • Transports across the nephron cells in this region starts with two basic driving forces: (Fig. 26-12) • 1. Osmosis: Having higher concentration of water in the filtrate than in the interstitial fluid. • 2. Active Na+/K= exchange pump at the site of basal membrane to force Na+ out of the cell to the interstitial fluid. • Thus, water will go back to the nephron blood vessels, peritublar capillary, by osmosis. • Na+ gets out from the nephron cells to the interstitial fluid by the Na+/K+ exchange pump.
Most of the ions, glucose and amino acids from the filtrate will enter the nephron cells in the form of Na+ cotransport, since the intracellular Na+ concentration is constantly being lowered by Na+/K+ exchange pump. At the site of the basal membrane, they will diffuse out, sometimes facilitated, according to the concentration gradients. Reclaims 60 - 70% of water and most of the glucose (diabetes mellitus?), amino acids and other organic substances. Urea, uric acid and creatinine are not absorbed, thus increasing their concentrations in the tubule.
(a) The loop of Henle (Fig. 26-13) • The descending portion of the loop of Henle reabsorbs additional 20% of water by osmoais and small amounts of ions may be returned to the filtrate. • On the contrary, the ascending portion of the loop of Henle, which is impermeable to water, reabsorbs 25% of sodium and chloride ions. by the Na+/K+ exchange pump locate in the basal membrane - similar to the proximal tubule. • In fact, the sodium and chloride ions absorbed back into the interstitial fluid contribute to extract more water from the descending portion of the loop. • NOTE: Pumping of ions across a cell
We have already seen that cell membrane may have a sodium pump which is energized with ATP. If the cell membrane is uniform over the entire cell, sodium may simply pumped out from the cell, but the sodium ion cannot run across the cell. To transport Na+ across a cell, requires a cell with asymmetirc membrane. Proximal tubules and ascending loop of Henle are surrounded with such cells. In the membrane towards the interstitial space, sodium ion is actively transported out from the cell into the interstitial space. While on the tubular side of the membrane, in which no active sodium pump is found, sodium ion, along with the others, passively enters into the cell. The over all movement of sodium ion is to actively transport from the tubular to interstitial fluid across the cell.
The results of active pumping of the salts in the ascending loop of Henle are in two fold:(1) The salt concentrations in the upper end of the tubule go down.(2) The salt concentrations in the upper region of medulla will go up due to the released salts. The consequence of increased salt concentrations in medullar will result in more effective osmotic release of water from the tubule. By the time the urine leaves the loop of Henle, it has much lower concentrations of Na+ and Cl-. By this time 80% of water and 85% of the solutes have been reabsorbed. The waste products are not reabsorbed.
(a) The distal convoluted tubule (DCT) and the collecting system • The DCT and collecting duct are impermeable to solutes. • Requires active reabsorption or secretion for transport. • Active reabsorption of Na+ is exchanged for K+ or H+ in response to aldosterone. Fig. 26-14, 15
The water reabsorption is controlled by antiduretic hormone (ADH). (Fig. 26.17of Seeley) ADH activate ADH receptor and in turn activates G-proteins for cAMP production, which opens up the water channel in the membrane, thus removes water out of the urine. At the end of the distal collecting duct, the solution osmolarity could increase from 100 mOSM at the entrance to 1200 mOSM
a. The control of kidney function • By adjusting the diameters of the afferent and efferent arterioles. • Activities of the sympathetic division of the ANS. • Via hormonal control.
i. The local regulation of kidney function • By automatic changes in the diameters of the arterioles and the glomerular capillaries - change in the blood pressure. • ii. Sympathetic activation and kidney function • By adjusting the flow of blood to the kidneys. • Sympathetic activation results in constricting the afferent arterioles - reduced blood flow to the glomerular capillaries. • Sympathetic activation of the vasomotor center changes the regional pattern of blood circulation - reduced GFR.
ADH: The function of ADH has been discussed earlier. (Fig. 26.17 of Seeley) Insufficient release of ADH may result in diabetes insipidus, large quantity of clear urine accompanied with dehydration and abnormal electrolyte balance. In contrast, diabetes mellitus may result in large quantity of urine with high concentration of glucose.
Renin -Angiotensin II- Aldosterone system for Na+, Cl- and K+ balance. (Fig. 26.18 of Seeley) Decrease in the concentration of Na+ in the interstitial fluids increase the rate of aldosterone secretion initiating the release of Na+ from the distal tubule.
1. Urine transport, storage and elimination • c. The micturition reflex and urination • The process of urination is coordinated by the micturition reflex. Fig. 26.20 • Note the stretch receptor - sensory fiber - parasympathetic motor neurons etc. • 200 ml of urine in the bladder sends the urge starting from the stretch receptors. • Contraction and relaxation of the internal and external sphincters decide the release of urine.
CHAPT 27: Water, Electrolytes and acid base balance • Extensive discussion on fluid, electrolytes and acid-base balance are presented in this chapter. We will focus only on acid base balance based on carbonic acid.
1. Acid and base • Most commonl definition of acid is its ability to produce H+. • There are strong and weak acids. • Strong acids dissociate completely to ions and produce H+ and the counter ions. Examples are • HCl -- H+ + Cl- • H2SO4 –- 2H+ + SO4= • On the other hand, weak acids dissociate partially and establish equilibrium. Examples are acetic acid and carbonic acid.
2. Buffers and acid base balance Buffers are substances which resist the change of pH a solution and a weak acid is a good candidate. In human body, proteins and carbonic acid take the major role as buffers. The buffering action of proteins depend ionization of groups, which may be ionized at physiological range of pH, 7.2 - 7.4. Such compounds are the alpha amino group and histidine of proteins. R-NH3+ = R-NH2 + H+