Sinusitis: Causes, Symptoms, and Management
E N D
Presentation Transcript
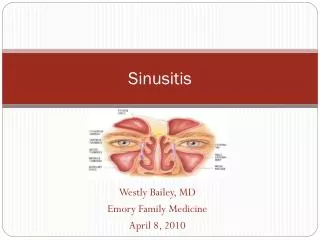
Anatomy • Paranasal Sinuses
Sinuses • The sinuses are hollow air-filled sacs lined by mucous membrane. The ethmoid and maxillary sinuses are present at birth. The frontal sinus develops during the 2nd year of life and the sphenoid sinus develops during the 3rd year.
Sinuses – types Four pairs of paranasal sinuses • Frontal-above eyes in forehead bone • Maxillary-in cheekbones, under eyes • Ethmoid-between eyes and nose • Sphenoid-in center of skull, behind nose and eyes
Sinuses have small orifices (ostia) which open into recesses (meatus) of the nasal cavities. • Meatus are covered by turbinates (conchae). • Turbinates consist of bony shelves • There are 3 turbinates and 3 meati in each nasal cavity (superior, middle, and inferior).
Sinusitis • Inflammation of the mucosal lining of paranasal sinuses
An acute inflammatory process involving one or more of the paranasal sinuses. • Occurs when the ostia from the sinuses are narrowed or blocked by inflammation or hypertrophy of the mucosa • Maxillary and ethmoid sinuses are most frequently involved.
Causes • Bacterial sinusitis – streptococcus pneumoniae, hemophilusinfluenzae, beta hemolytic streptococci, klebsiella, pneumoniae • Viral sinusitis – rhinovirus, influenza virus, adenovirus • Fungal sinusitis – aspergillus and candida
Risk factors • Allergies, nasal deformities, cystic fibrosis, nasal polyps, and HIV infection. • Respiratory tract infection • Cold weather • Day care attendance • Smoking in the home
Pathopysiology • Usually follows rhinitis, which may be viral or allergic. • May also result from abrupt pressure changes ( diving) or dental extractions or infections. • Inflammation and edema of mucous membranes lining -the sinuses leads to obstruction of the sinuses
With inflammation, the mucosal lining of the sinuses produce mucoid drainage. Bacteria invade and pus accumulates inside the sinus cavities. • If the sinus orifices are blocked by swollen mucosal lining, the pus cannot enter the nose and builds up pressure inside the sinus cavities. • Signs and symptoms
Classification • Acute Sinusitis – respiratory symptoms last up to four weeks • Subacute sinusitis – respiratory symptoms last between 4 to 12 weeks • Chronic sinusitis – respiratory symptoms last more than 12 weeks .
Complications of Sinusitis • Cellulitis or abscess • Meningitis • Brain abscess • Wheezing in children with asthma
Signs and symptoms -Sinusitis • Pressure, pain, or tenderness over sinuses • Low-grade temperature, Malaise • Persistent nasal discharge, often purulent • Postnasal drip- upper airway cough syndrome • Cough, worsens at night • Mouthing breathing, snoring • Sore throat, bad breath • Headache • Nasal congestion, nasal obstruction • Acute sinusitis – hyperemic and edematous mucosa, discolored purulent nasal drainage and enlarged turbinates
Diagnostic Tests • History collection • Physical examination • X ray • Sinus CT, MRI • Nasal endoscopy – to examine the sinuses, obtain drainage for culture and restore normal drainage • Rhinoscopy – fiberoptic examination of the nose
Management Antibiotics-treat for 10-14 days, depending upon severity, with one of the following: • Amoxicillin:20-40mg/kg/d in 3 divided doses(>20kg, 250mg tid) • Augmentin:25-45mg/kg/d in 2 divided doses(>20kg, 400mg bid)
Biaxin (clarithromycin):15mg/kg/d in 2 divided doses • Cefzil:15mg/kg/d in 2 divided doses • Lorabid (loracarbef): 30mg/kg/d in 2 divided doses
Codeine (antitussive) – for severe pain and cough • Rhinocort nasal spray – 2 sprays in each nostril every 12 hours for children over 6 years of age. • Acetaminophen or ibuprofen to relieve pain • Decongestants – relieve nasal congestion • Antihistamines
Non-pharmacological treatment • Humidifier to relieve the drying of mucous membranes associated with mouth breathing, steam inhalation • Increase oral fluid intake 6 to 8 glass of water • Saline irrigation of the nostrils • Moist heat over affected sinus • Prolonged warm shower to promote drainage • Do not smoke or avoid exposure to smoke
Saline solution can be prepared at home • 1/4 tsp of salt dissolved in 8 oz of tap water . A pinch of baking soda may be added • 3 times daily
Surgical management Functional endoscopic sinus surgery (FESS) • Uses Fiberoptic endoscope • Diseased tissue which is located by CT scan will be dissected • If surgery is doing with local anesthesia, patient is only kept for 2-3 hours postoperatively and then discharged • This will promote sinus drainage and ventilation and remove diseased tissue and also opens ostia • This can be also used for the removal of polys, foreign bodies
CALDWELL – LUC sinus operation • Also known as radical antrum operation - It is a radical operation to the maxillary sinus performed through the oral vestibule • Incision under the upper lip • Surgeon removes part of anterior bony wall of the maxillary sinus, producing a permanent window • The diseased tissues are dissected and drained. • Antrum or cavity may be packed to prevent bleeding • Packing removed after 24 to 48 hours after surgery • As the maxillary sinus heals, the exposed bone is covered by mucosa
Ethmoidecotmy • Removal of enthmoid air cells • Diseased mucosa, nasal polyps or mucocele are removed • Mucocele – mucous cyst that leads to repeated infection • Ethmoidectomy is performed in 3 ways – transnasal, transantral and external
Sphenoid sinus surgery • Endoscopic technique • External or transantral approach • Removes ethmoid sinus and opens the anterior wall of the sphenoid sinus • Diseased tissue is removed along with mucus membrane lining the sinus.
Frontal sinusectomy • OSTEOPLASTIC FLAP OPERATION • Complete removal of diseased mucosa of the frontal sinus and for obliteration of the sinus so that it is no longer functional or continuous with the inner nose. • Obliteration is done with subcutaneous fat obtained from the left lower abdominal quadrant
Nursing management Pre operative teaching • NPO for 6-8 hours before surgery • Explain that the patient will: • receive a sedative , feel pressure not pain during surgery • Have a nasal pack for 24 to 48 hours after surgery • Have a mustache dressing after surgery • Have black eyes and swelling around nose and eyes for 1 to 2 weeks • Feel pressure, not pain during surgery
Post operative teaching Precautions for the first week • After general anesthesia, position the patinet in side line. • Do not blow nose atleast 3 to 5 days after surgery • After caldwellluc operation do not blow nose for 2 weeks • Tell the patinent to expectorate secretion instead of swallow • Try not to sneeze, Do not bent over • Avoid constipation, Maintain Oral hygiene
Encourage mid fowlers position when fully awake to promote drainage and decrease edema • Apply ice compresses over nose • Encourage liberal fluid intake
Managing pain – acetaminophen Taking care of drainage – bright red bleeding is expected for a week • Change the pad several time each day depending on the amount of drainage • After initial bloody drainage stops, a thicker, yellowish green drainage may continue for several weeks
Breathing difficulties • Keep the head elevated • Sleep with an extra pillow- more comfort, decrease edema and allow better drainage • Cool mist humidifier usage
Rest and activity • Avoid strenuous activities • After a week swimming, jogging are permitted • If bleeding occurs, stop activity • Avoid heavy lifting Self monitoring • Report signs of infections • Expect ecchymosis for 1 – 2 weeks • Expect tarry stools from swallowed blood for a few days • Avoid aspirin which can cause bleeding