Download
1 / 17
200 likes | 515 Views
Disorders of the face and scalp. Prepared by Mick Svoboda Presented by Dr. Cardinal. Acneiform eruptions. Acne fulminans - severe cystic acne w/ ulcerating cysts. Commonly on chest/back of young males. Pyoderma faciale - inflammatory cystic acne on the central face of young women.

E N D
Disorders of the face and scalp Prepared by Mick Svoboda Presented by Dr. Cardinal
Acneiform eruptions • Acne fulminans- severe cystic acne w/ ulcerating cysts. Commonly on chest/back of young males. • Pyoderma faciale- inflammatory cystic acne on the central face of young women. • Dissecting cellulitis- inflammatory and scarring ds. of the scalp and neck. Begins w/ boggy nodules that form sinus tracts. • Acne keloidalis- perifollicular inflammatory disorder of the scalp resulting in keloids.
Seborrheic dermatitis • Erythema and waxy scaling of skin folds and hair-bearing areas of the face, scalp, and groin. • Tx. • Antidandruff shampoos containing zinc (Head and Shoulders) or selenium (Selsun Blue) • Face involvement- low potency hydrocortisone cream (1-2.5%), Short duration 3-5 days.
Erysipelas and facial cellulitis • Erysipelas • more superficial than cellulitis. • Group A strep most likely pathogen • Facial cellulitis • Staph spp. And Strep spp. Most likely pathogens. • Clinical features • Hot, erythematous, tender, extends peripherally . • Tx. • Inpatient IV abx if necessary. • Ophtho. consult if orbit involved.
Herpes zoster infection • Pain/dysthesia precedes rash 3-5 days. • Involvement of the ophthalmic branch of the CN V is of concern. Risk for HZO. • Suspect Ramsay Hunt syn. if rash in external auditory canal/TM • Diag. by Tzanck smear or viral cx. Usually not necessary. • Tx. • Antivirals helpful if given w/in 72hrs after eruption. • Possibly shorten duration/decrease pain of postherpetic neuralgia, • analgesics
HSV • Most commonly type 1. • Typical HSV lesions (painful, grouped vesicles w/ red base). • Primary eruption usually gingivostomatitis. • Recurrent HSV presents as herpes labialis “cold sores” • Tx. • Primary gingivostomatitis • Mild disease- symptomatic tx only. • Moderate to severe or immunocompromised - antivirals • Recurrent HSV • Antivirals not required.
Cutaneous Lupus Erythematosus • Acute • Classic malar/ butterfly rash. • Often assoc. with systemic sxs of SLE, which helps in differentiating from other facial rashes (ex. rosacea, dermatomyositis, etc.). • Chronic • Referred as discoid lupus erythematosus. • Results in scarring and pigmentary changes most commonly in AA males. • Only 10% assoc. w/ systemic sxs of SLE. • Commonly occurs in photodistributed areas.
Photosensitivity disorders • Sunburn • Erythema/warmth to sun exposed area- 1st degree burn. Presence of blisters- 2nd degree burn. • Tx • Protection from sun exposure. • NSAIDS • Exogenous photosensitivity disorders • Topical photosensitizers • Cutaneous rash (similar to sever sunburn) at site of application • Furocoumarins most common offending agents (lime juice, parsnips, celery, figs). • Ingested photosensitizers • Rash at all sun-exposed areas • Lasix, tetracyclines, sulfonamides, amiodarone. • Tx.- if possible remove offending agent.
Contact dermatitis of the face • Aerosolized allergens • Diffuse erythema w/ or w/out vesiculation. • Ex. Rhus- aerosolized allergens from burning of poison ivy/oak. • Direct contact allergens • Most prominent on sensitive skin such as eyelids. • Ex. Nickel, nail polishes, tooth paste, make-up preservatives. • Tx. • avoiding the offending agent. • Topical (low potency/short duration) or oral steroids if severe.
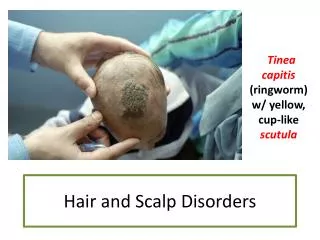
Hair loss • Tinea capitis • Dermatophyte inf. • Alopecia w/ broken hair follicles and scales in the periphery. • Patchy, usually nonscarring. • May have kerion- boggy, tender, indurated plaque w/pustules. • Tx • Griseofulvin 15-20mg/kg d PO w/ meals for 6-8 weeks. • Can add Nizoral shampoo. • Close contacts should be evaluated.
Alopecia Areata • Nonscarring patchy hair loss. • Affected area is bald and no inflammation or scaling present. • Differential • Hyperthyroidism • Secondary syphilis • Telogen Effluvium • Hair loss related to stressful events (pregnancy, major surgery/illness). • Occurs 2-3 mos after insult.
Scalp and forehead lacerations • Evaluation- assess for depth, laceration of the galea, depressed skull fx. • Scalp repair • Not necessary to shave or cut hair. Increases rate of wound inf. • Large galeal defects - 4-0 nonabsorbable sutures. • Muscle layers - 4-0 absorbable sutures. • Skin- staples or simple interrupted nylon.
Forehead repair • Deep structure handled similar to above. • Skin – 6-0 nonabsorbable sutures. • If skin under tension- 5-0 intradermal absorbable sutures. • Make sure to approximate skin tension lines and hairline. • Eyebrow repair • Make sure to line up hair margins. • As w/ scalp it is helpful to leave tails long and use a different color than the pts. hair to assist removal. • Disposition • Wound care instructions. • Sutures/staples removed • Scalp- 7-10 days • Forehead/face- 3-5 days
Eyelid lacerations • Evaluation • Check integrity of the globe • Check for corneal abrasion, FB, or damage to surrounding structures of the eye. • Require ophtho f/u if involves • lid margin • inner surface of lid • Lacrimal duct • Associated ptosis • Extends into tarsal plate • Repair/disposition • Closure w/ 6-0 or 7-0 nonabsorbable suture. • Small bites avoiding deep penetration through the lid. • Sutures removed in 3 days.
Nose lacerations • Evaluation • Inspect for septal hematoma. • If assoc. w/ blunt injury, rhinorrhea may indicate cribriform plate fx. • Repair/disposition • Superficial lacs- close skin with 6-0 monofilament. • Through-and –through lacs- place a 5-0 suture aligning the alar rim. • Mucosal layer is closed next w/ absorbable 5-0 suture. • Reirrigate from outside and close w/ 6-0 as above. • Sutures removed in 3-5 days. • Septal hematomas require drainage.
Lip lacerations • Repair • Infraorbital block and mental nerve block for upper and lower lip lacs respectively. • Isolated intraoral lacs- may not require closure. • Through-and-through- closed in layers 1) Mucosa 2) Orbicularis oris muscle 3) Skin • Vermilion border involved- first stitch should align this. • Pt w/intraoral sutures should be placed on prophylactic abx (PCN).
Ear lacerations • Evaluation • blunt mechanism of injury check for • Integrity of TM, especially if lac extends into canal. • Subchondral hematoma- • Otorrhea • Repair • Can use auricular nerve block. • Superficial- • 6-0 monofilament • cover exposed cartilage and don’t remove any pieces of cartilage. • Through-and-through- • If gaping- one or two 6-0 nonabsorbable sutures to approximate cartilage • Following repair a pressure dressing can be used to control bleeding.