Download
1 / 130
1.3k likes | 1.33k Views
Enhance your skills in pediatric resuscitation with this comprehensive lecture focusing on rapid cardiopulmonary assessment, recognition of respiratory distress and failure, and shock progression. Learn about various conditions, survival rates, and assessments to ensure efficient care in emergencies.

E N D
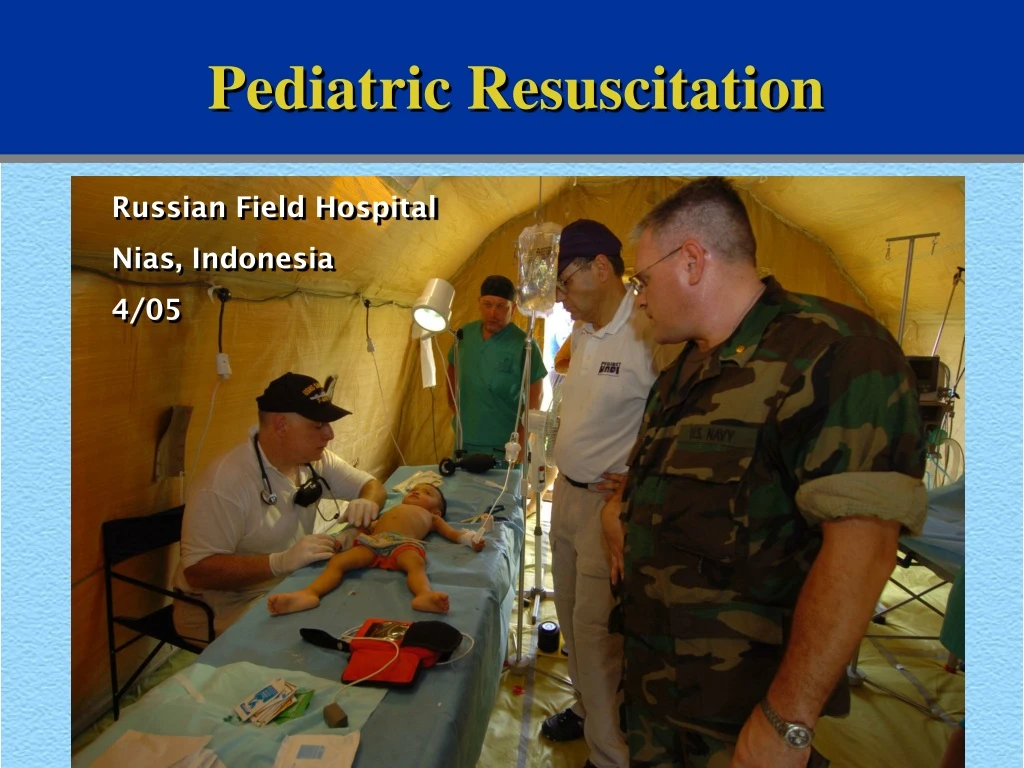
Pediatric Resuscitation Russian Field Hospital Nias, Indonesia 4/05
Lecture Objectives The goal of this module: • Perform rapid cardiopulmonary assessment • Recognize signs of respiratory distress, respiratory failure, and shock
Progression of Respiratory Failure and Shock Various Conditions Respiratory failure Shock Cardiopulmonary failure Cardiopulmonary arrest
Comparison of Survival 100% Survivalrate 50% 0% Respiratoryarrest Cardiopulmonaryarrest
Rapid Cardiopulmonary Assessment 1. Evaluation of general appearance (mental status, tone, responsiveness) 2. Physical examination of airway, breathing, and circulation (ABCs) 3. Classification of physiologic status Rapid cardiopulmonary assessment should be accomplished in less than 30 seconds!
Evaluation of General Appearance • General color (“looks good” vs “looks bad”) • Mental status, responsiveness • Activity, movement, muscle tone • Age-appropriate response
Physical Examination: Airway • Clear • Maintainable • Not maintainable without intubation
Evaluating Respirations • Respiratory rate • Respiratory effort (work of breathing) • Breath sounds/air entry/tidal volume • STRIDOR (inspiration) • WHEEZE (expiration) • Skin color and pulse oximetry
Rapid Cardiopulmonary Assessment:Classification of Status • Respiratory distress:Increased work of breathing • Respiratory failure:Inadequate oxygenation or ventilation
Blood pressure Cardiovascular VariablesAffecting Systemic Perfusion Preload Myocardial contractility Afterload Stroke volume Heart rate Cardiac output Systemic vascularresistance
Response to Shock 140 100 60 20 Vascular resistance Percent of control Blood pressure Cardiacoutput Compensated shock Decompensated shock
Decompensated Shock Compensatory mechanisms fail to maintain adequate cardiac output and blood pressure
Physical Examination: Circulation • Cardiovascular function • Heart rate • Pulses, capillary refill • Blood pressure • End-organ function/perfusion • Brain • Skin • Kidneys
Physical Examination: Circulation Typical Assessment Order: • Observe mental status • Feel for heart rate, pulse quality, skin temperature, capillary refill • Measure blood pressure • (Measure urine output later)
Physical Examination: Circulation Evaluation of responsiveness • A — Awake • V — responsive toVoice • P — responsive toPain • U — Unresponsive
Heart Rates in Children Infant 85 220 300 Normal Compensating? SVT Child 60 180 200 Normal Compensating? SVT
Physical Examination: Circulation Evaluation of skin perfusion • Temperature of extremities • Capillary refill • Color • Pink • Pale • Blue • Mottled
Capillary Refill Prolonged capillary refill (10 seconds) in a 3-month-old with shock
Physical Examination:Circulation Estimate of Minimum Systolic Blood Pressure Age Minimum systolic blood pressure (5th percentile) 0 to 1 month 60 mm Hg >1 month to 1 year 70 mm Hg 1 to 10 years of age 70 mm Hg + (2 age in years) >10 years of age 90 mm Hg
Physical Examination:Circulation • Cardiovascular function • Heart rate • Pulses, capillary refill • Blood pressure • End-organ function/perfusion • Brain (Mental Status) • Skin (Capillary Refill Time) • Kidneys
Physical Examination: Circulation Evaluation of End-Organ Perfusion Kidneys • Urine Output • Normal: 1 to 2 mL/kg per hour • Initial measurement of urine in bladder not helpful
Classification of Physiologic Status: Shock Early signs (compensated) • Increased heart rate • Poor systemic perfusion Late signs (decompensated) • Weak central pulses • Altered mental status • Hypotension
Septic Shock Is Different • Cardiac output may be variable • Perfusion may be high, normal, or low • Early signs of sepsis/septic shock include • Fever or hypothermia • Tachycardia and tachypnea • Leukocytosis, leukopenia, or increased bands
Special Situations: Trauma • Airway and Breathing problems are more common than Circulatory shock • Use the ABC or assessment triangle approach plus • Airway + cervical spine immobilization • Breathing + pneumothorax management • Circulation + control of bleeding • Identify and treat life-threatening injuries
Special Situations: Trauma Spinal Precautions? Pneumothorax? Bleeding control?
Special Situations: Toxicology • Airway obstruction, Breathing depression, and Circulatory dysfunction may be present • Use the ABC and assessment triangle approach, plus watch for • Airway: reduced airway protective mechanisms • Breathing: respiratory depression • Circulation: arrhythmias, hypotension, coronary ischemia • Identify and treat reversible complications • Administer antidotes
Special Situations: Toxicology Is the Patient Awake enough to maintain airway? Respiratory Effort and Rate? Arrythmias? Vascular Tone? Ischemia?
Classification of Physiologic Status: Cardiopulmonary Failure Cardiopulmonary failure produces signs of respiratory failure and shock: • Agonal respirations • Bradycardia • Cyanosis and poor perfusion
Classification of Cardiopulmonary Physiologic Status • Stable • Respiratory distress • Respiratory failure • Shock • Compensated • Decompensated • Cardiopulmonary failure
Rapid Cardiopulmonary Assessment: Summary • Evaluate general appearance • Assess ABCs • Classify physiologic status • Respiratory distress • Respiratory failure • Compensated shock • Decompensated shock • Cardiopulmonary failure • Begin management: support ABCs
Checkpoint • Rapidly perform assessment • Use the information to prioritize your resuscitation efforts • Remember the Pediatric Assessment Triangle as we practice cases
Rapid Cardiopulmonary Assessment Application A 3-week-old infant arrives in the ED: • CC: Severe vomiting and diarrhea • Physical exam: Gasping respirations, bradycardia, cyanosis, and poor perfusion What ar the results of your RAPID ASSESSMENT? What is the PHYSIOLOGIC STATUS? What are the emergency interventions?
Rapid Cardiopulmonary Assessment Application Case Progression • Response to intubation and ventilation with 100% oxygen: • Heart rate: 180 bpm • Blood pressure: 50 mm Hg systolic • Pink centrally, cyanotic peripherally • No peripheral pulses • No response to painful stimuli What is happening? What is next treatment step?
Rapid Cardiopulmonary Assessment Application: Response to Therapy • Vital signs improved
Pediatric Intubation Andrew Garrett, MD Division of Transport and Emergency Medicine
Goals • Review of some basic concepts of pediatric airway management • Introduce/review RSI in a stress-free environment • Have a chance to practice intubation skills later today
Review and Overview of Airway Management • Children at higher risk for hypoxia and respiratory failure: • Anatomic differences • Higher metabolic rate • Ambiguous symptoms of hypoxia • Head trauma is common in pediatrics • Limited practice of management skills
Airway Anatomic Differences (Extrathoracic) • Relatively larger tongue • Tongue placed superiorly (C3-4) • Angle of epiglottis angled away from larynx • Vocal folds can trap ET tube • Narrowest area at cricoid vs. glottis
Anatomy epiglottis True VC False VC cartilage trachea esophagus
Airway Anatomic Differences(Intrathoracic) • Compliance of conducting airways at high flow rates • Fewer, smaller alveoli (< 8 yrs) • Smaller FRC (functional reserve) • Decreased diffusion • Metabolic Rate • 2 x adult oxygen consumption rate • Shorter tolerance of apnea