Download
1 / 10
100 likes | 548 Views
Clinical Pathology Conference. May 21, 2018 Jody Manners, PGY4. Clinical History. 50 year old female with history of EtOH abuse, NHL s/p R-CHOP 2005, headaches, transferred with AMS. LSW 6pm on 4/28, presented to OSH after found at 2pm on 4/29 “unresponsive” and with agonal breathing

E N D
Clinical Pathology Conference May 21, 2018Jody Manners, PGY4
Clinical History • 50 year old female with history of EtOH abuse, NHL s/p R-CHOP 2005, headaches, transferred with AMS. • LSW 6pm on 4/28, presented to OSH after found at 2pm on 4/29 “unresponsive” and with agonal breathing • At OSH, emesis and aspiration and eventually intubated on arrival in Presby ED
Additional History • PMH: EtOH abuse, NHL s/p R-CHOP 2005, headaches • PSH: Hysterectomy • Home meds: lorazepam, metoprolol • ROS: per family, several days of severe HA
Exam • OSH: • Hypothermic, reported fixed pupils • At PUH: • HR 76, BP 162/100, RR 24, T 29.5 • Intubated without sedation, 4/4 TOF • Pupils 6mm fixed, symmetric. • +R corneal, no cough, +gag • Extension in all extremities
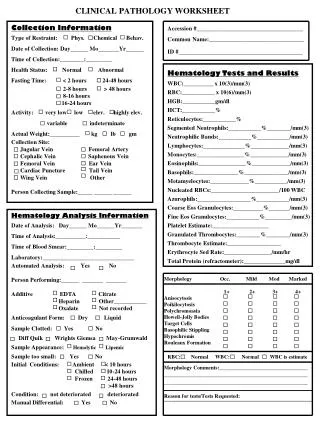
Labs • Na 131, BUN/Cr 6/0.3, glucose 115 • WBC 8, Hb 15, plt 251 • Lactate 3.2 • CPK 1029 • Trop < 0.10 -> 0.37 • EtOH 35
Imaging Final Read • Large R SDH, 1.8cm subfalcine herniation, brainstem duret hemorrhage + IVE in 4th, early/subacute R PCA infarct involving parietal/posterior mesial temporal and entrapment of R temporal horn and left lateral ventricle
Hospital Course • NRSGY evaluation in the ED; no intervention and suspected poor prognosis. • Admitted to 4G where expected progression to brain death would occur. • Slowly rewarmed with monitoring of electrolytes, pressor support • Family focus on comfort on 4/29-4/30 • CTB 4/30
Autopsy Findings: • Severe calcific atherosclerotic cardiovascular disease, up to 95% occlusion of proximal LAD, healed posterior LV infarct, cardiomegaly (440g) and LVH • Bronchopneumonia • Hepatomegaly with steatosis (suspected related to EtOH abuse) • Horseshoe kidney joined at lower poles with focal cortical hemorrhage, with incidental focus of renal cell carcinoma (grade 2, clear cell type favored) • No evidence of lymphoma
Gross Examination of Brain • Expected Gross findings • Suspected etiology?