Chronic Infections of the Larynx
310 likes | 1.2k Views
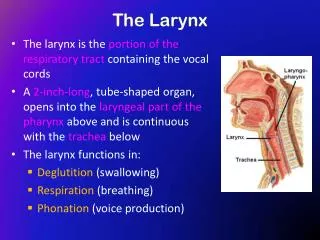
Chronic Infections of the Larynx. - Dr Subhodh H R. Chronic laryngitis Reinke’s edema Pachydermia larynges Atrophic laryngitis TB larynx Lupus of the larynx Syphilis of larynx Leprosy larynx Scleroma larynx. Chronic Hyperaemic laryngitis. Inflammation Without hyperplasia

Chronic Infections of the Larynx
E N D
Presentation Transcript
Chronic Infections of the Larynx - Dr Subhodh H R
Chronic laryngitis • Reinke’sedema • Pachydermia larynges • Atrophic laryngitis • TB larynx • Lupus of the larynx • Syphilis of larynx • Leprosy larynx • Scleroma larynx
Chronic Hyperaemic laryngitis • Inflammation Without hyperplasia • Symmetrically involved inflammation of laryngeal subsites
Etiology • Following acute simple laryngitis • Other foci of head and neck infection. Eg: PNS, tonsils, teeth etc • Occupational factors. Eg: miners, strokers, gold & iron smiths, chemical factory workers • Smoking and alcohol • Chronic lung diseases • Vocal abuse
Clinical features • Hoarseness – commonest • Early fatigability of voice • Constant hawking • Discomfort in throat • Chronic cough • ILS : • Hyperaemia • Dull red and rounded cords • Flecks of viscid mucus on cords and inter-arytenoid region
Treatment • Eliminate other foci of infection • Avoid irritants ( smoking, alcohol, dust & fumes ) • Voice rest and speech therapy • Steam inhalation • Expectorants ( mucolytics )
Chronic hyperplastic laryngitis • Inflammation with hyperplasia • Maybe diffuse or localised • Localised variety presents as: dysphonia plica ventricularis, reinke’sedema, vocal nodules, vocal polyp, contact ulcer
Etiology: similar to Chronic hyperplastic laryngitis • Pathophysiology: • Begins in the glottis as hyperemia+edema and spreads around. • Mucosa, submucosa, glands, intrinsic muscles and joints are involved • Squamous metaplasia and hyperplasia with keratinisation • Mucous glands undergo hypertrophy initially and later atrophy
Clinical features • Predominantly Males • 30- 50yrs • Symptoms similar to chronic hyperaemic variety • ILS: • Dusky red mucosa and thickened. • Red swollen vocal cords, look irregular • Bulky false cords • Mobility maybe impaired due to oedema and infiltration, and muscle atrophy and CA joint arthritis.
Treatment • Conservative management as in Chr. Hyperaemic laryngitis • Surgical: • Vocal cord stripping – removing the hyperplastic mucosa • Damage to underlying vocal ligament be avoided • One side operated at a time
Reinke’s edema • Middle age • Bilateral symmetrical swelling of the membranous part of the vocal cords • Edema in the subepithelial space • Due to chronic irritation – voice misuse, smoking, LPR, chronic sinusitis, myxoedema
Clinical features: • Hoarseness – low pitched rough voice • ILS: • Fusiform appearance of the vocal cords with pale look • Hyperaemic and maybe hypertrophic false cords • Treatment: • Decortication of the vocal cords on one side and 3-4 weeks later on the other sides • Voice rest • Speech therapy
Pachydermia laryngis • Chronic hypertrophic laryngitis affecting the posterior part of larynx in the region of inter arytenoid and posterior part of the vocal cords
Cl/ F: • Husky voice • Irritation in the throat • ILS: • Red and grey granulation tissue in the inter arytenoid region and posterior thirds of the vocal cords • Contact ulcers • Bilaterally symmetrical • Treatment: • Microlaryngoscopic excision • Acid reflux treatment • Speech therapy
Atrophic laryngitis • Laryngitis sicca • Atrpohy of the laryngeal mucosa with crust formation • Common in women • Associated with atrophic rhinitis and pharyngitis
Cl/ f: • Intermittent hoarseness of voice due to crusts • Dry irritating cough • Occasional dyspnoea • ILS: • Atrophic mucosa • Foul smelling crusts • Excoriation and bleeding on removal of crusts • Maybe seen spreading along the trachea • Treatment: • Elimination of the cause • Humidification • Glucose in glycerine sprays • Expectorants
Tuberculosis of larynx • Almost always secondary to pulmonary TB • Middle aged males • Bronchogenic or haematogenic route of spread • Affects mainly posterior larynx: • Inter arytenoid fold • Ventricular bands • Vocal cords • epiglottis
Cl/f: • Weakness of voice • Hoarseness • Pain radiating to ears( ulceration ) • Dysphagia and odynophagia
ILS : • Hyperaemia with limited adduction • Mamillated inter arytenoid region • Mouse nibbled vocal cords ( ulceration ) and inter arytenoid regions • Granulation tissue • Turban epiglottis ( pseudoedema ) • Swollen false cords and AE folds • Surrounding pallor
Diagnosis: • X ray chest • Sputum examination • DL scopy biopsy • Treatment: • Voice rest • Anti TB drugs as for Pulmonary TB
Lupus larynx • Indolent tubercular infection associated with lupus of nose and pharynx • Involves the anterior part of the larynx • Epiglottis is commonly affected and maybe completely destroyed • Progresses downwards • Generally asymptomatic as it is painless • Diagnosed incidentally on routine examination in case of lupus of nose • Good prognosis with Anti TB drugs
Laryngeal syphilis • Rare • Gumma of tertiary stage maybe seen • May present as a smooth swelling which may ulcerate later • Diagnosis by biopsy and serology • Laryngeal stenosis may be a complication
Leprosy of the larynx • Rare • Associated with leprosy of nose and skin • Diffuse nodule over the epiglottis or AE fold or arytenoids • May ulcerate later • Diagnosis by biopsy • Deformity of the laryngeal inlet and stenosis are the complications
Scleroma larynx • Klebsiellarhinoscleromatis • Associated with nasal involvement • Smooth red swelling in the subglottis • Hoarseness, wheezing and dyspnoea • Diagnosis by biopsy • Treatment: • Streptomycin • Steroids • Subglottic stenosis is a complication