Download
1 / 8
80 likes | 377 Views
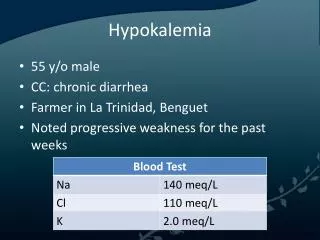
Hypokalemia - initial diagnosis and treatment. MMH A1 施孟甫. H. y. p. o. k. a. l. e. m. i. a. &. P. a. r. a. l. y. s. i. s. H. y. p. o. k. a. l. e. m. i. a. &. P. a. r. a. l. y. s. i. s. +. K. excretion rate and acid. -. base status ?. +. +. +.

E N D
H y p o k a l e m i a & P a r a l y s i s H y p o k a l e m i a & P a r a l y s i s + K excretion rate and acid - base status ? + + + L o w K e x c r e t i o n a n d High K excretion and L o w K e x c r e t i o n a n d n o r m a l a c i d - b a s e abnormal acid - base n o r m a l a c i d - b a s e Acid - base state ? Hyperthyroidism ? YES NO Metabolic Acidosis Metabolic Alkalosis + NH excretion Blood pressure TPP l 4 (UAG, UOG) Normal High Low High GS or BS Primary Diuretics mineralocorticoid excess Toluene Clue RTA Vomiting Profound diarrhea R enin Aldo Renin Renin Aldo Aldo Primary Licorice use None Family history Hypernatremia Aldo steronism AME Ectopic ACTH SPP FPP Hypernatremic HPP l l l Liddle syndrome Barium poisoni ng l Lin SH et al. Am J Emerg Med 2003 (
Low Renin Low Aldosterone Cortisol Low High Normal Liddle’s Licorice AME DOC Ectopic ACTH Cushing syndrome 11 b hydorxylase D 17 a hydorxylase D Lin SH, et al. Am J Med Sci 2003; 325: 153-156.
How to supply K • Decrease 1 meq/L means deficient 200~400 meq K • Check the Osmolarity and Acid-base status, especially DKA and acidosis will mask the K deficient condition • Don’t use sugar content IVF • Cl • Every bottle< 20 meq KCl, except femoral line is available
Summary • Please collect urine before supplement • Check Serum: Na, K, Cl, Ca, P, Mg, BUN, Cr, Osmo, Ht, Hct, (P,抽完先請檢驗室離心處理檢體否則cell lysis 會影響數據) • Check Urine:Na, K, Cl, P, Ca, Mg, Cr, Osm, (uric acid, Urea, protein) • Check Blood gas: vein is also OK • 如有 elevated GOT, please check CPK • We are always available !!!