Download
1 / 9
100 likes | 279 Views
Hematocrit During the Cardiopulmonary Bypass: Impact on Clinical Outcome During Ascending Aortic Surgery. SF Zhou MD 1 , AL. Estrera MD 2 , T Pawelek MD 1 , C Ignacio MD 1 , S Panthayi MD 1 , MD; K Shebaclo BS 1 , H Safi MD 2 , R Sheinbaum MD 1. Department of Anesthesia 1

E N D
Hematocrit During the Cardiopulmonary Bypass: Impact on Clinical Outcome During Ascending Aortic Surgery SF Zhou MD1, AL. Estrera MD2, T Pawelek MD1, C Ignacio MD1, S Panthayi MD1, MD; K Shebaclo BS1, H Safi MD2, R Sheinbaum MD1 Department of Anesthesia1 Department of Cardiothoracic and Vascular Surgery2 The University of Texas Medical School at Houston Memorial Hermann Heart & Vascular Institute
Introduction • Blood transfusions worsen clinical outcomes in aortic surgery. • Hemodilutional anemia increases organ ischemia risk. • We show the lowest hematocrit (Hct) that reduces transfusion and prevents hemodilution associated complications.
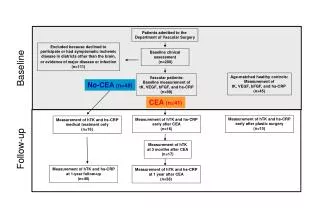
Methods We reviewed 399 cases of Ascending Aortic (Aneurysm or Type A dissection) repair with deep hypothermic circulatory arrest (DHCA). Demographics and surgical characteristics (except age) were similar between groups. Patient ages were 17-89 and are grouped by Hct <16%, <18%, 19%-20%, 21%-22%, > 23% at temperature < 20C, 20-28C, 28-32C, 32-34C, 34-35C during CPB.
Methods Databases were established by collecting medical information through patient medical records and 2010 ICD-9-CM Volume 1 Diagnosis Codes, including complications of surgical and medical care, not elsewhere classified 996-999 and diseases of the specific system or organ. The data analysis was by mean ( standard deviation) for continuous variables and by frequency (percentage) for qualitative variables. Two-sample t-test or Chi-Square test was used to compare groups with P-value of less than 0.05 considered significant.
Results • Changes in outcome were suggested at Hct <16% versus >16% at <20C during DHCA and also for Hct <18% versus>18% at temperature 20-28 C. • Risk of ARF and postoperative tracheotomy increased with Hct < 16 (Table 2). • Chance of discharge home improved with higher Hct at all temperatures (Table 3). Mortality decreased at Hct 21-22% at 20-34C and increased at Hct <16% during DHCA (Table 4).
Conclusion Patient temperature affects oxygen demand, blood viscosity, oxygen carrying capacity and delivery. Hct value is a transfusion trigger and should change with body temperature during aortic surgery. Hct 21-22% appears favorable for CPB at 20-34C. Hct <16% during DHCA increases mortality. Hct <18% during rewarming (20-32C) increases postoperative ARF risk.