Download
1 / 34
340 likes | 359 Views
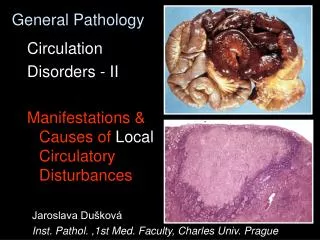
Learn about amyloidosis, a disorder of protein metabolism characterized by abnormal extracellular deposition of proteinaceous material. Explore its history, classification, clinical manifestations, and diagnostic methods.

E N D
General Pathology Amyloidosis Fibrinoid, Hyalin Jaroslava Dušková Inst. Pathol. ,1st Med. Faculty, Charles Univ. Praguehttp://www1.lf1.cuni.cz/~jdusk/
Amyloidosis DEF.: disorder of protein metabolism accompanied with abnormal extracellular deposition of proteinaceous material - amyloid
Amyloid = starch like Amyloid - history Karl Freiherr von Rokitansky (1804-1878) Rudolf Ludwig Karl Virchow (1821-1902).
Amyloid - history 2. Karl Freiherr von Rokitansky (1804-1878) Austrian pathologist, born February 19, 1804, Königgrätz, Böhmen, Austrian Empire(now Hradec Králové, East Bohemia, Czech Republic); died July 23, 1878, Wien. Handbuch der pathologischen Anatomie IInd Band, Wien 1842
Amyloidosis – morphology Macroscopy: • small amounts – invisible • larger deposits – enlarged, firm, waxy organs
Ultrastructure & Biochemistry of Amyloid 90-95% non branched fibrils diam. 10-12nm 5-10% p-component - glycoprotein + fibronectin, laminin, collagen 4
Amyloidosis conformational disease (Carrell and Lomas, Lancet, 1997) „…arises when a constituent protein undergoes a change in size or fluctuation in shape with resultant self - association and tissue deposition“ pleated β – sheet structure
Conformational diseases (Carrell and Lomas, Lancet, 1997) • Amyloidosis • Prionoses - transmissible spongiform encephalopathies (incl. m. CJD) • m. Alzheimeri pleated β – sheet structure
Amyloidosis Classification: • according to the source protein (more than 20 different identified) • according to the distribution • systemic (generalised) • localised
Systemic Amyloidosis - I. AL - imunocyte dyscrasia associated light chains Ig (mostly )„primary“ Distribution: tongue, heart, GIT, liver, spleen, kidney Associated diseases: Plasma cell myeloma, B cell lymphoma,
Systemic Amyloidosis - II. AA - reactive systemic amyloidosis SAA = Serum Amyloid Associated protein„secondary“ Distribution: liver, kidney, spleen, GIT, lymph nodes, bowel, adipose tissue Associated diseases: rheumatoid arthritis, chronic infections (tb, leprosy, bronchiectasiae, osteomyelitis, IBD, neoplasms MLH , RCC
Systemic Amyloidosis - III. senile systemic SSA 25% people over the age of 80 years (!) • normal transthyretin TTR (prealbumin) • mostly heart & vessels invilvement
Systemic Amyloidosis - IV. A2 - hemodialysis associated 2 microglobulin Hereditary AA - Familial Mediterranean Fever ATTR - Famil. polyneuropatia transthyretin (mutated form)
Systemic Amyloidosis - complications diminished functions of some organs, esp. KIDNEY FAILURE IIIrd stage Amyloid nephrosis
Localised Amyloidosis - I. Senile cardial ATTR - transthyretin - (structurally normal) Senile cerebral A - -amyloid protein
Cardiac Amyloidosis – clinical manifestations • Dilated Cardiomyopathy (predominant systolic dysfunction) • Restrictive cardiomyopathy (predominant diastolic dysfunction) • Congestive heart failure • Rhytm abnormalities • Coronary insufficiency • Valvular dysfunction • Pericardial tamponade • Enhance sensitivity to digitalis glycosides • Atrial thrombosis - embolisation
Localised Amyloidosis - II. Endocrine ACal - ca medullare gl. thyreoideae AIAPP - islets of Langerhans associated AANF - isolated atrial amyloidosis atrial natriuretic polypeptide Nodular tumoriform amyloid deposits (tongue, lung,larynx, skin, urinary bladder, orbita)
Clinical Diagnosis of Amyloid Scintigraphy (in vivo) using human serum amyloid component marked with 123J Echocardiography (atrial amyloid)
Clinical Diagnosis of Amyloid Biochemistry sequening DNA -hered. forms extraction of fibrils (from a biopsy specimen) spectrometry sequening of the amyloid protein
Amyloidosis – morphology Macroscopy: • small amounts – invisible • larger deposits – enlarged, firm, waxy organs
Morphological Diagnosis of Amyloid Macroscopy • reaction Virchow I (sol. Lugolli) Virchow II (H2SO4)
Microscopy: KONGO red (+POLARISATION!) + KMnO4 thioflavine S,T crystal. violet (metachromasia) IMMUNOHISTOCHEMISTRY(electron microscopy) Morphological Diagnosis of Amyloid
Materials: GIT (stomach, duodenum rectum, gingiva) biopsy kidney sural nerve & muscle fat aspiration biopsy – needle with an internal diam. 0,7-1,2mm Morphological Diagnosis of Amyloid Röcken Ch. Sletten K.: Amyloid in Surgical Pathology Virchows Arch., 2003, 1-26
synthesized by young chemist at Bayer comp. 1883 as the first of economically lucrative direct (nod needing a mordant) textile dyes patented by AGFA 1885 (Aktiengeselschaft für Anilinfarbenfabrikation) 3 weeks after the conclusion of the West Africa Conference to Europeans in 1885, the word Congo evoked exotic images of far-off central Africa known as The Dark Continent the Congo red stain was named „Congo“ for marketing purposes by a German textile dyestuff company in 1885 CONGO Red Steensma DP: „Congo“ Red. Out of Africa? Arch. Pathol.Lab.Med.,2001, 125, 250-2
Reversibility of Amyloid • The deposits are NOT irreversible. e.g.Hrncic R. et al: Antibody mediated resolution of light chain – associated amyloid deposits. Am.J. Pathol., 2000, 157,12369-46 • Progression of generalised amyloidosis can be delayed or stopped by treatment of the underlying disease. Röcken Ch. Shakespeare Ann: Pathology, diagnosis and pathogenesis of AA amyloidosis. Virchws Arch. , 2002, 440, 11-122
Prevention & Therapy of Amyloid • Prevention & treatment of the underlying diseases • Vaccination against β am. protein in mice diminished senile plaque formation and improved memory. Nature Medicine, 2001, 7, 18th Jan. • A β –based experimental therapies based on degrading enzymes. Zlokovic et al.: Neurovascular Pathways and Alzheimer Amyloid β-peptide. Brain Pathol. , 2005, 15, 78-83
Fibrinoid & Hyalin disorders of protein metabolism
Fibrinoid Change of Collagen • vessels and connective tissue damage • plasmorrhagia (leakage of plasma) • deposits of Ag-AB complexes • staining characteristics fibrin - like
Hyaline change Definition (historical, descriptive): intra- or extracellular change of homogenous rose „ glassy“ appearance in the H&E stained histological sections
Hyaline change Extracellular: corpus albicans, scars, hyalinoses of serous membranes Intracellular: Crooke cells, Mallory´ hyaline, Russell bodies
Ultrastructure • Fibrinoid - collagen fibres surrounded by plasma proteins may be reversible • Hyalin – collagen fibres increased in thickness, changed architecture rather stable
Hyaline change Extracellular: corpus albicans, scars, hyalinoses of serous membranes Intracellular: Crooke cells, Mallory´ hyaline, Russell bodies
Significance of Fibrinoid Change • diminished quality of the collagen ( firmness, permeability) • tendency to thrombosis in the vessels, aneurysms formation
Significance of Hyalin Change • diminished quality of the collagen ( elasticity) • ischemia in organs with thickened arterial walls • intracellular - function, death