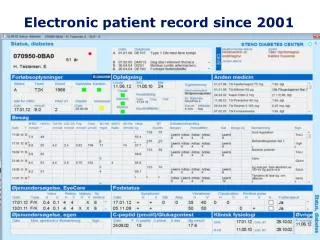
Electronic patient record
Electronic patient record. Records. A record is a group of separate related data fields/elements that form a single unit information. A record may be of fixed length or variable length, depending on the computer and the method and type

Electronic patient record
E N D
Presentation Transcript
Electronic patient record
Records A record is a group of separate related data fields/elements that form a single unit information. A record may be of fixed length or variable length, depending on the computer and the method and type of storage media. A fixed-length record allows a fixed number of spaces for a field or data element; a variable-length record takes only the spaces it actually needs. • Fixed-length record • Not flexible • Not efficient • Programs to process them are easier to be prepared • Cost less • Variable-length record • Flexible • Store data more efficiently • Difficult to prepare computer programs using them • Cost more
Patient Record The patient record is the major document that contains data about the patient’s health care. It is used by all the providers of health care services to record, store, and review information. Patient Record System A patient record system is the set of components that form the mechanism by which patient records are created, used, stored and retrieved. The patient record may be a paper-based patient record or an electronic patient record (computer-based).
The purpose of Healthcare Records (1) The purpose of the Healthcare Record itself is faithfully to preserve the information recorded in it. This implies that a Healthcare Record must support different purposes as: Patient purposes • make available information about the patient • make available information to the patient • protect the patient rights regarding their clinical and personal information Professional purposes • improve the capacities to reach a diagnosis, to state a prognosis and to prescribe an adequate therapy • provide a legal context for the collection of the data • enable each care provider to authenticate their entry by signature Ethical purposes • serve the needs of the ethical context • provide data which is sufficient for the purpose
The purpose of Healthcare Records (2) Management purposes • provide data for management at different levels of the care system Statistics and Research purposes • provide information about the disease episode • provide a means for cumulative information about specific diseases and programmes • aid in the optimisation of technologies for care Training purposes • provide data for training Third party financial purposes • meet the requirements of Insurance companies who are partly or completely paying for care • meet the requirements of Communes and Government organisations paying for care • meet the requirements for audit of the care system at any level CEN/TC251/PT011/N300/V.1.00
The Uses of the Healthcare Record The information in the HR may be used for a variety of purposes: Patient purposes • For the diagnosis, prognosis, treatment and follow-up of the patient • For planning and defining the care for the patient • To ensure continuity of disease prevention and diagnosis, prognosis, and treatment Professional purposes • As a diary for the providers of care • For protection of professionals • For audit of the providing of care/quality control • For efficient and effective providing of care • For day to day management of the care system Management purposes • For providing the best quality of care • As a basis for measuring resource use by the patient • For billing when required • For planning of the care system Statistics and Research purposes • For statistics/research at any level in the care system Training purposes • For trainining or updating clinical skills Third-party financial purposes • To meet the requirements of Insurance companies who are partly or completely paying for care • To meet the requirements of Communes and Government organisations paying for care • To meet the requirements for audit of the care system at any level
Paper-Based Patient Record (1) Paper-based patient records differ from hospital to hospital, and in some hospitals from patient unit to patient unit, as well as varying for the different types of health care facilities providing patient care. It is also difficult to process and access information in paper-based patient records.
Paper-based Patient Records (2) The pros: 1. Paper patient records are familiar to users who consequently do not need to acquire new skills or behaviours to use them. 2. Paper records are portable and can be carried to the point of care. 3. Once in hand, paper records do not experience downtime as computer systems do. 4. Paper records allow flexibility (lack of standard vocabulary and coding) in recording data and are able to record “soft” (i.e. subjective) data easily. 5. Paper records can be browsed through and scanned (if they are not too large). This feature allows users to organise data in various ways and to look for patterns or trends that are not explicitly stated.
Paper-based Patient Records (3) The cons: 1. Problems with Patient Record content (missing, illegible, excessive, redundant or inaccurate data) 2. Problems with format (data are fragmented within the record and not sorted for relevance, usually are organised according to the sources and chronology of data) 3. Problems with access, availability and retrieval 4. Problems with linkages and integration (discontinuity of care among providers) 5. Problems with outpatient records (are great in number, scattered among individual physisian offices and usually exhibit even greater variance in quality)
Critical issues to be considered 1. The uses of and legitimate demands for patient data are growing. Part of this growth can be attributed to increased concern about the content and value of clinical therapies and a recent intense focus on health services research. 2. Powerful and affordable technologies to support computer-based patient records are now available. 3. Increasingly, computers are being accepted as a tool for enchancing efficiency in virtually all facets of everyday life. 4. Demographic such as an ageing population (which results in a growth in chronic diseases) and the continued mobility of the population create greater pressures for patient records that can manage large ammounts of information and are easily transferable among health care providers. 5. Pressures for reform in health care are growing, and automation of patient records crucial to achievement of such reform.
Electronic Patient Record Automation provides a solution to many information gathering and dissemination problems and can be used to more effectively and efficiently provide data for outcomes research Dick and Steen, 1991 The advantages of the electronic patient record are: • More effective use of resources • Improved access • Reduces cost • Enhances research • Improves care
Electronic Patient Record Architecture • A health record shall be regarded as a logical data structure being • composed of the following contsructs: • items • items complexes • representing the content and the context of information in the • healthcare record CEN/TC 251/PT 011/N 300 V.1.00
Data structures • A structure of only one record item complex • Tree structure (a data structure composed solely of original record item complexes and a query record item complexes • Directed acylic graph structure (the structural links of the View record item complexes extend the pure tree structure into a directed graph structure)
Record item A record item is a construct that shall be used for the representation of a healthcare record entry or a component of a healthcare record entry where all such components are regarded as constituting meaningful quantities of information when considered alone. A record item shall be composed of a set of attributes that expresses some characteristics of the item. CEN/TC 251/PT 011/N 300 V.1.00
Record item attributes 1. The content attributes of record items capture the healthcare datathemselves. 2. Each record item should have only oneorigin attribute specifying the original record item complex regarded to be its original information context. 3. The unique record item instance identifier attribute. 4. The record item name. 5. Revised version attribute: Each record item may have attributes providing references that link successive versions of an amended record item. 6. Each record item may have attributes establishing the status of the record item (e.g. valid, modified, invalid.) 7. Subject of care identification: Each record item shall relate to the subject of the record. 8. Date and time of recording. 9. Agent recording attribute (identifying the healthcare enterprise agent that recorded the content) 10. Agent responsible for the record item content. 11. Signature. 12. Date and time of the signature. 13. A record item may have one or more comment attributes. 14. A record may have additional attributes (references).
Example of the Record item attributes Let’s consider Jane Smith’s visit to City Health Centre December 12, 1993 for a fracture of femur: • In this record, the diagnosis “Fracture of femur” • is an example of an entry that can be regarded as a • record item. In this case, “Fracture of femur” • would constitute thecontent attribute of the • record item. • The content of the record item in this example • is not sufficient to correctly interpret it, it is • necessary to know what the entry really is, whom • it concerns, who recorded it, when was recorded, • etc. All this is represented by the attributes of the • record item e.g.: • attributes covering reference to the place in the record to which a record item is considered to “belong” e.g. origin, instance identifier, revised version, status. • attributes to identify the content e.g. name • attributes to describe the organisational context in which the content was recorded. City HC Jane Smith 561224-1234 #2 931212 pH Diagnosis: Fracture of the femur Family history: Both parents died from myocardial infarction Patient history: Fell on slippery pavement in Oslo yesterday… Status: Examination of the right leg shows….etc.
Record item complex Record item complexes are constructs that shall be used for the representation of the structures of records. The record itself must be regarded as a record item complex. A defined set of records, e.g. the set of records belonging to an electronic healthcare record system, may be regarded as a record item complex. A record item complex shall be composed of a set of attributes that expresses some characteristics of the record item complex.
Record item complex attributes (1) 1. Record item complex type: A record item complex shall be of one of the following types: Original, View, Query 2. Record item complex content: The content must be of the following type dependent on its type: * An original record item complex shall contain zero or more record items and zero or more record item complexes. * A view record item complex shall contain one or more references. * A query record item complex shall contain one or more criteria for the selection of record items from the record. 3. Origin: Each complex shall have only one origin attribute specifying the original record item complex. The original record item complex reffered by this attribute shall be regarded as its parent node in the data structure. 4. Unique record item complex instance identifier: Each complex should be uniquely distinguishable. 5. Record item complex name. 6. Revised version: Each complex may have attributes providing references that link successive versions of an amended record item complex. 7. Status (e.g. valid, modified, invalid). 8. Presentation (may have one or more presentation attributes) 9. Data organisation: how the content of the complex is organised (e.g. sequentially, alphabetical, chronological, increasing, decreasing).
Record item complex attributes (2) 10. Subject of care identification: Each record item complex shall relate to the subject of the record. 11. Date and time of recording: Each record item complex shall have the date and time of recording 12. It Healthcare enterprise Agent recording. 13. Healthcare enterprise Agent responsible for the record item complex content. 14. Signature (may have a signature of the agent responsible) 15. Date and time of the signature. 16. Comment (may have one or more comment attributes) 17. Additional attributes (these include additional attributes containing references to concepts of conceptual models).
Original record item complex View record item complex Jane Smith 561224-1234 Careplan #1 Medical Diagnosis Fracture of femur: City HC Jane Smith 561224-1234 #2 Nursing Problems Difficulties managing activities of daily living Anxiety for her heart Fear for how to manage home 931212 pH Diagnosis: Fracture of the femur Family history: Both parents died from myocardial infarction Patient history: Fell on slippery pavement in Oslo yesterday… Status: Examination of the right leg shows….etc. Goals In three weeks Mrs Smith is able to take care of daily activities With professional help Mrs. Smith can recover whithout fear for her heart Inter- ventions Home health care nurse helps Mrs. Smith in the first days 2 hours mornings and evenings using: - Activity therapy - Emotional support - Rehabilitation exercises - Self care assistance - Training activities in daily living Nursing Record Medical Record Fracture of femur Content of a record item
The Healthcare record item complex City HC Jane Smith 561224-1234 #2 City HC Jane Smith 561224-1234 #1 931201 ZP Diagnosis: Heel spur syndrome Family history: Both parents died from myocardial infarction Patient history: Experiensed pain under heel when shovelling snow.. Status: Examination of ...etc 931212 pH Diagnosis: Fracture of the femur Family history: Both parents died from myocardial infarction Patient history: Fell on slippery pavement in Oslo yesterday… Status: Examination of the right leg shows….etc. The set of items that, for some reason, is regarded as constituting a unit in a particular HR, is called a Healthcare record item complex.
A Healthcare record described by the basic construct of the record architecture Symbols: Coneptual models: data model terminology coding sceme Architecture terms: Attribute making a Reference Healthcare record item Healthcare Original record item complex View Query Conceptual models Partial description of the architectural aspects of the structure of one (instance of a) HR
(1) The objectives of a standard electronic healthcare record architecture • To make possible the improvement of health care quality and the better use of resources • To facilate the conformance of HRs to the ethico-legal practices and other policies applicable • To facilitate safe understandable communication between different electronic healthcare record systems and with other computer-based systems in the healthcare environment used for other purposes • To facilitate safe understandable communication between electronic healthcare record systems and healthcare professionals • To facilitate the changing of electronic healthcare record systems while keeping the data • To promote competition between systems vendors and between health care providers • To promote open systems, based on common components, data output, interfaces, structure and data access • To improve productivity of the Information Technology industry and quality of the software, and enlarge the healthcare software market • To facilitate the free movement of patients by improving the portability of the healthcare record • To promote the use of common conceptual models, terminology and definitions. Thus, the architecture must...
(2) Thus, the architecture must • be compliant with other architectures within the healthcare framework • promote healthcare records suitable for the clinical purposes in a closed or open clinical environment for private or public systems of care • facilitate inter-working among various healthcare enterprises for the benefit of the patient • increase the security and safety of operations on the information in the record (both for the person in question and for the healthcare professionals) • satisfy the domain requirements of the healthcare professionals • permit the representation of different kinds of content, including text, coded information, images, graphics and sound • enable the representation of context information • enable the healthcare record to operate in theappropriate ethico-legal environment • enable the operations on the record to be audited by the person in question, by the user of the record or by a competent third party, if required • enable each entry, decision, prescription or any other order to be appropriately signed by each legal responsible person, if required • facilitate the convergence of different terminology • facilitate new functions of healthcare record systems, adapted to clinical circumstances, management requirements, system needs, and advancing technology • facilitate the interchange of records • facilitate the tracking of the assembly of a healthcare record and its sub-components during active use • ensure that the archived record is a safe and proper assembly of its components and subcomponents provide a means for the safe control of copying one or more sections of the record and for regulation of the lifetime of those topics
Critical issues to be considered Maintaining Confidentiality There is the absolute necessity to protect the patient privacy by protecting the principle of confidentiality - the obligation of health care professionals to avoid violating a patient’s right to privacy. A significant challenge in creating future patient record systems is to achieve an appropriate balance between confidentiallity and access by users with a need to know.