Download
1 / 22
220 likes | 646 Views
Also known as c. diff. CDI CDAD Anna Alvarez 4/22/2010. Clostridium Difficile. C. difficille. gram + anaerobic bacillus found in the gut. flourishes when normal host microflora is inhibited by antibiotic use. Antibiotics mild to severe. Leading cause of infectious diarrhea in the U.S.

E N D
Also known as c. diff. • CDI • CDAD Anna Alvarez 4/22/2010 Clostridium Difficile
C. difficille • gram + anaerobic bacillus found in the gut. • flourishes when normal host microflora is inhibited by antibiotic use. • Antibiotics • mild to severe
Leading cause of infectious diarrhea in the U.S. • $ 2, 871 - $ 4, 846 – treatment of primary C diff. • $ 13, 655 - $18, 067- treatment of 1 recurring case of C diff. • Ghantoji, S.S., Sail,K., Lairson, DR. Dupont, HL, & Garey, K.W.( 2010) . Background
Annual incidence- > 250, 000 nosocomial cases with a mortality rate of 1- 2.5%. • Annual cost of C diff in the US is between $750 million - $ 3.2 billion. • Elevated costs are due to multiple hospitalization and medications. • LOS 18.0 days vs. 4.0 ( CDI vs. Non CDI) • Ghantoji, S.S., Sail,K., Lairson, DR. Dupont, HL, & Garey, K.W.( 2010) . Background cont
10 day course of medication Metronidalizole = $26.42 Vancomycin = $ 863 - $1160 Ghantoji, S.S., Sail,K., Lairson, DR. Dupont, HL, & Garey, K.W.( 2010) Cost of Medication
Multiple and prolonged antibiotic use penicillin, clindamycin, cephlasporins and fluoroquinolones( resistant form of C diff) • Immunocompromised- elderly, postop CV, DM, Renal disease, CA, HIV, transplant • Owens, R.C., Donskey,C.J.,Gaynes, R.P., Loo,V.G.& Muto,C., (2008). At risk POPUlations ( Common)
Subjective history: foul smelling stools, greater than 3-6 watery stools within 24 hours. abdominal pain previous treatment with antibiotics dehydrated Kelly, C.P. & LaMont, T. ( 2008) Symptoms ( mild Case)
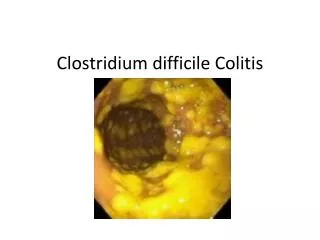
Positive stool culture for toxin producing C diff. • Endoscopy: pseudomembranes noted, + toxin assay for toxin A/B . Diagnosis
D/C triggering antibiotic • Rehydration with IV fluids • 10 day oral course of Vancomycin or Metrodianizole treatment
Signs and symptoms of an acute abdomen abdominal pain, hypotension, elevated lactic acid, tachycardia, renal failure • Endoscopy: patches of pus sloughing , killing normal bowel. Severe Cases – pseudomembranaous colitis
Toxic Megacolon • Medical emergency 32 – 80% mortality rate • Surgical intervention( exploratory laparotomy, subtotal colectomy, ileostomy) • Vancomycin and Metronidazole via N/G., or pr. • Al-Abed, Y.A., Gray, E.A. & Rothnie, N. D., (2010) Kelly, C.P. & LaMont, T. ( 2008)
Increased production of toxins A/B • Bind to colon tissue, release toxins • Responsible for major outbreaks • Recurrering infection • Kelly, C.P. & LaMont, T. ( 2008) North American Pulsed Field( NAP-1/027)
Stool Transplantation • Family member • Stool screened for communicable diseases. Recipient treated with Vanco prior to the transplant • Stool was instilled via N/G tube and flushed with 25cc of NS. • No recurrence was noted. • Aas, C., Gessert, C. E., & Bakken, J., S. ( 2003). New Treatment!!
Spore transmission through contact. • Spores live on object • Asymptomatic carriers of C diff spores. • Infection control measures • Bleach, isolation, disposable equipment, hand washing • Ghantoji, S.S., Sail,K., Lairson, DR. Dupont, HL, & Garey, K.W.( 2010) Community Acquired C Diff
Pt/Family identify those at risk pt’s at risk for C diff/fulminating colitis encourage physicians to change to po meds as soon as possible teach pt / family – isolation, washing hands Role of the CNS
Nurses • Adhere to appropriate isolation • Help nurses recognize those pt who are most at risk for further decline. CNS Role cont:
Systems Monitor infection rates and collaborate with infection control , environmental. CNS ROLE CONT:
Aas, J. Gessert, C.E., & Bakken, J.S. ( 2003) Recurrent Clostridium difficile colitis: Case series involving 18 patients treated with donor stool administered via a nasogastric tube. Clinical Infectious Diseases, 36, 580-585. Al-Abed- Y.A., Gray, E.A. & Rothnie, N.D. (2010). Outcomes of emergency colectomy for fulminant Clostridium difficile colitis. The Surgeon, 330-333. Ghantoji, SS, Sail, K., Lairson, D.R., DuPont, H.L., & Garey, K.W.( 2010). Economic healthcare costs of Clostridium difficile infection: a systematic review. Journal of Hospital Infection, 74 309-318. Kelly, C. P., La Mont, T. ( 2008). Clostridium difficile- more difficult than ever. New England Journal of Medicine. 359, 1932- 1940. . References
Owens, R.C., Donskey,C.J.,Gaynes, R.P., Loo,V.G.& Muto,C., (2008). Antimicrobial-associated risk factors for clostridium difficile infection. Clinical Infectious Disease, 46, S19- 2 31 References