Download
1 / 48
480 likes | 933 Views
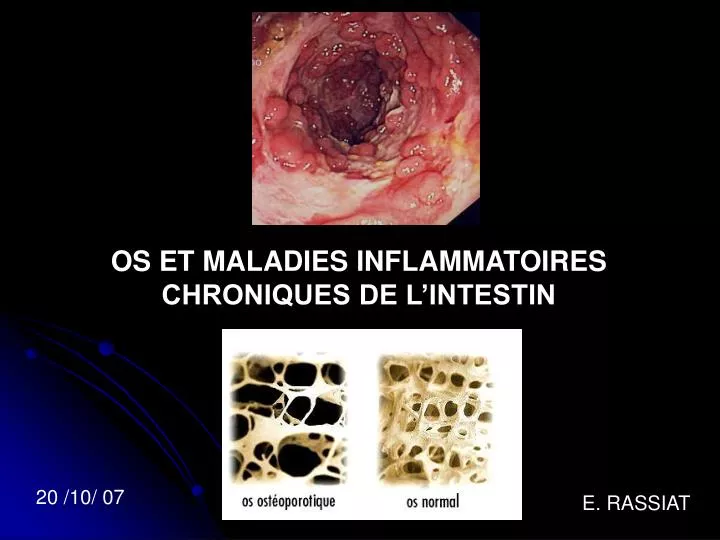
OS ET MALADIES INFLAMMATOIRES CHRONIQUES DE L’INTESTIN. 20 /10/ 07. E. RASSIAT. MICI . ATTEINTES EXTRA DIGESTIVES : OS , ARTICULATIONS ++ PEAU FOIE, VOIES BILIAIRES ORL ŒIL POUMONS (RCH) VASCULAIRES. Ca 2+, Mg, Phosphates Collagènes,

E N D
OS ET MALADIES INFLAMMATOIRES CHRONIQUES DE L’INTESTIN 20 /10/ 07 E. RASSIAT
MICI ATTEINTES EXTRA DIGESTIVES : OS , ARTICULATIONS ++ PEAU FOIE, VOIES BILIAIRES ORL ŒIL POUMONS (RCH) VASCULAIRES
Ca 2+, Mg, Phosphates Collagènes, Cellules osseuses Tissu vivant, en constant renouvellement
ATTEINTES ARTICULAIRES périphériques axial OSTEOPENIE OS AUTRES sapho, ostéonécrose, tendinopathie, iatrogène OSTEOPOROSE
ATTEINTES ARTICULAIRES • 25 à 30% des malades • Arthralgies >> arthrites • Arthropathies périphériques (8 à 20%) • Atteinte axiale (5 à 10 %) : pelvi-spondylite • ou rhumatisme axial • Avant, pendant , après la 1ère poussée • 5 % des malades sont • durablement touchés
ATTEINTES ARTICULAIRES PERIPHERIQUES ARTHRITE ARTICULATION ROUGE, CHAUDE, DOULOUREUSE, AUGMENTEE DE VOLUME
Arthropathies PERIPHERIQUES (8 à 20%): • Toutes les articulations • mono, oligo, poly arthrites • - Aigues + • Oligo arthrites migratrices, non destructrices • grosses et petites articulations des extrémités • Membres inférieurs = Genoux, chevilles++ • Poignets, métacarpo-phalangiennes • Facteur rhumatoïde, auto-anticorps négatifs • Plus fréquent pour CROHN / RCH • -Plus fréquent si atteinte colique ?
Arthropathies PERIPHERIQUES (8 à 20%): 2 Types = TYPE 1 = moins de 5 articulations atteinte asymétrique, aigue (90%) évolution parallèle aux poussées digestives(80% souvent avec érythème noueux, uvéite TYPE 2 = plus de 5 articulations atteinte symétrique, bilatérale atteinte chronique(88%) évolution indépendante des poussées digestives (65%)
Arthropathies périphériques (8 à 20%): TRAITEMENTS: traitement des poussées digestives (cf type 1) Antalgiques (paliers I , II) AINS efficace mais risque toxicité intestinale (RR=2 aggravation MICI) Sulfalazine (Salazopyrine) Sulfalazine , corticoïdes (20 à 40 mg/j) , methotrexate, infliximab
ATTEINTES AXIALES (5 à 10%) Sacro-iliite ++(4 à 18%) atteinte unilatérale, prédominance féminine lombalgie basse matinale, douleur fesse avec raideur, déverrouillage, HLA B27 négatif séries scintigraphies : 50 %, asymptomatique Spondylarthrite ankylosante (1 à 8%) douleurs rachidiennes matinales, raideur réduction mobilité rachis, atteinte capacité respiratoire, crohn=rch HLA B27 : 50 à 75%, Sex-ratio=2
ATTEINTES AXIALES (5 à 10%) Sacro-iliite ++(4 à 18%) Spondylarthrite ankylosante (1 à 8%) Evolution indépendante / MICI+++(durée, gravité, type, complications) Précèdent le diagnostic de MICI = 50% Evolution chronique
SACRO ILLIITE IRM > TDM >Radio Scintigraphie osseuse
ATTEINTES AXIALES (5 à 10%) TRAITEMENTS: Kinésithérapie, rééducation rachidienne Antalgiques (paliers I, II) AINS efficace mais risque toxicité intestinale Sulfalazine+ Sulfalazine (3 à 6g/j) , corticoïdes (> 40 mg/j) methotrexate ? infliximab+++
AUTRES LESIONS = Ostéonécrose aseptique hanche corticoïdes, alcool,traumatisme homme 30 à 50 ans ischémie osseuse IRM++ SAPHO = synovite, acné, pustulose palmoplantaire, psoriasis hyperostose, ostéite aseptique Hippocratisme digital (15 % rch - 38% crohn) corrélé à la fibrose intestinale déformation doigts
AUTRES LESIONS = • Ostéonécrose aseptique hanche (corticoïdes, IRM) • SAPHO = synovite, acné, pustulose palmoplantaire, psoriasis • hyperostose, ostéite aseptique • Hippocratisme digital (15 % rch - 38% crohn) • corrélé à la fibrose intestinale • Enthésiopathie = tendinite d’achille, plantaires , 6% MICI • Iatrogènes = tendinite (quinolones) • arthrite lupique ou sérique (infliximab, ciclosporine, • azathioprine) • arthrite septique (immunosuppresseurs)
ATTEINTES ARTICULAIRES périphériques axial OSTEOPENIE AUTRES sapho, ostéonécrose, tendinopathie, iatrogène OSTEOPOROSE
OSTEOPOROSE Maladie diffuse du squelette caractérisée par une diminution de la masse osseuse et des altérations de la micro architecture du tissu osseux, ayant pour conséquence une augmentation de la fragilité osseuse et du risque de fracture Conf de consensus 1993 ORIGINE MULTIFACTORIELLE ++
OSTEOPOROSE Baisse naturelle : 0.5 à 1% / an homme 1 à 2%/ an femme
OSTEOPOROSE et MICI Os : tissu en évolution constante, vivant ostéolyse ostéoformation Diminution de l’ostéoformation+++ L’ostéoporose est cliniquement latente avant la fracture
OSTEOPOROSE Atteinte diffuse , silencieuse fréquente : 150 000 fractures /an en France Fracture ostéoporotique : 40 % des femmes >50 ans 14% des hommes > 50 ans Le capital osseux se construit avant la puberté L’ostéoporose est cliniquement latente avant la fracture ORIGINE MULTIFACTORIELLE ++
OSTEOPOROSE Gènes Hormones oestrogènes, T3 Nutrition Ca2+, Vit D Age (max :20, 30 ans) Exercice physique Alitement, sédentarité Environnement TABAC++ alcool QUANTITE et QUALITE OS CORTICOIDES +++ INFLAMMATION +++ IL6 , CRP,TNF ORIGINE MULTIFACTORIELLE ++
OSTEOPENIE – OSTEOPOROSE-OSTEOMALACIE OSTEOPENIE= réduction de la masse osseuse OSTEOPOROSE = raréfaction osseuse ET une altération de la microarchitecture osseuse OSTEOMALACIE = défaut de minéralisation osseuse par carence Vit D (résection grêle, CSP, dénutrition, rare <5%, douleur cuisse, marche)
OSTEOPOROSE FRACTURE /TASSEMENT VERTEBRAL (65 ans) PERTE DE TAILLE, DOULEUR DE LA COLONNE VERTEBRALE
OSTEOPOROSE : FRACTURE (col fémur, radius) TASSEMENT VERTEBRAL Atteinte vertébrale : 2/3 asymptomatique ou quasiment ! (12% des femmes entre 50 et 80 ans ont >1 fracture Radiologique)
OSTEOPOROSE FRACTURE /TASSEMENT VERTEBRAL (65 ans) FRACTURE COL FEMORAL (70 ans)
OSTEOPOROSE FRACTURE /TASSEMENT VERTEBRAL (65 ans) FRACTURE COL FEMORAL (70 ans) FRACTURE DU POIGNET (55 ans)
OSTEOPOROSE DIAGNOSTIC CLINIQUE : DIMINUTION DE TAILLE FRACTURE DIAGNOSTIC RADIOLOGIQUE : TRANSPARENCE OSSEUSE (RX) OSTEODENSITOMETRIE
OSTEODENSITOMETRIE Mesure densité minérale osseuse (DMO) Faisceau de Rx Examen fiable, peu irradiant (1/10 rx poumon), simple, rapide Examen de référence pour mesurer la masse osseuse (rachis lombaire, fémur) Examen remboursé depuis 1/07/2006 - 70 %(39.9 euros) Diagnostic - suivi (délai >1 an ) Pas d’injection POSER LA QUESTION A VOTRE GASTRO+++
OSTEODENSITOMETRIE • 1- QUELQUE SOIT L’AGE, LE SEXE • Signes d’ostéoporose (tassement, fracture) • Corticoïdes > 3 mois, >7.5 mg/j • - Maladies hormonales : hyperthyroidie etc.. 2- FEMME MENOPAUSEE - ATCD familial 1° degré - Ménopause <40 ans - BMI < 19 kg/m2 - Corticoïdes > 3 mois, >7.5 mg/j
Diagnostic par Ostéodensitométrie(L2 L4 extrémité sup fémur) Score T est exprimé en référence au pic maximum de masse osseuse
Diagnostic par Ostéodensitométrie(L2 L4 extrémité sup fémur) OSTEOPENIE = T score <1 DS OSTEOPOROSE = T score < 2,5 DS OSTEOPOROSE SEVERE = T score < 2,5 DS et fracture
FACTEURS DE RISQUE OSTEOPOROSE= Antécédent familial 1°degré d’ostéoporose Caucasien, asiatique Sexe féminin Sédentarité Alitement Tabac++ (cf crohn) Alcool Café (>4) Cola (>3) Apport insuffisant ou malabsorption vit D , calcium
FACTEURS DE RISQUE OSTEOPOROSE= Dénutrition+++ Traitement = CORTICOIDE+++ héparine, anti épileptique Inflammation chronique +++ (IL 6, TNF, CRP ; IL4) Causes hormonales : ménopause,ménopause précoce, hypogonadisme, aménorrhée I ou II ,diabète, hyperthyroidie, hyperparathyroidie,insuffisance rénale, hémochromatose
OSTEOPENIE-OSTEOPOROSE ET MICI OSTEOPENIE=40 à 50% OSTEOPOROSE=6 à 14% OSTEOMALACIE = < 5 % (résection étendue grêle) Risque fracture faible RR=1,41 (rachis=2,2 ; fémur =1,59) , >60 ans Etude allemande sur 293 patients MICI= 53% ostéopénie, 15% ostéoporose, 34 tassements dont les 2/3 avant 30 ans CORTICOIDES >7,5 mg/j = perte osseuse de 7 % /an Attention dose cumulée = 30g
OSTEOPENIE-OSTEOPOROSE ET MICI Indication OSTEODENSITOMETRIE dans l’année du diagnostic= 1)atcd familial d’ostéoporose, fracture >50 ans tabagisme ménopause 2) corticoïdes > 3 mois
OSTEOPENIE-OSTEOPOROSE ET MICI PREVENTION+++ : éviter le recours et la durée des corticoïdes budésonide ou corticoïdes locaux soit immunosuppresseurs, infliximab sevrage tabac++(crohn) consommation alcool < 2/j consommation caféine <4/j (café, cola) alimentation (ca 2+ 1200 mg /j), activité physique hormonothérapie substitutive (gain 2% masse osseuse) Grande variabilité individuelle aux corticoïdes
OSTEOPENIE-OSTEOPOROSE ET MICI TRAITEMENT : OSTEOPENIE = calcium 1000 mg/j vit D= 500 à 800 UI/j augmentation de 4 % masse osseuse OSTEOPOROSE = idem et biphosphonates didronel actonel , fosamax > 4,6% masse osseuse après 1 an T score ≤ 1.5 diphosphonates à envisager ( HAS 2006)
BIPHOSPHONATES Inhibition de la résorption osseuse Ingestion le matin, à jeun, 30 minutes à 2 heures avant la prise d’aliments ou de calcium, ne pas s’allonger dans les 30 minutes Risque d’ulcérations oesophagiennes Prise prolongée dans le temps pour avoir une efficacité++ Didronel , Actonel, Fosamax, bonviva (150mg/mois) Contre indications : grossesse, allaitement, insuffisance rénale
Ranelate (proteos) Action sur la formation et la résorption osseuse 1 sachet 2g /j le soir au coucher 2 heures après le diner Prévention secondaire fracture ostéoporotique Prévention primaire si T score <3 ou <2.5 et facteur de risque : > 60 ans, ménopause précoce <40 ans , BMI <19 , corticothérapie ancienne ou actuelle à une posologie >7.5 mg /j Associé à vit D, Ca2+ Attention : quinolones, cyclines
CONCLUSIONS POSER LA QUESTION A VOTRE MEDECIN Douleur articulaire périphérique vertébrale Ostéodensitométrie ?? Traitement ostéopénie : vit D, Ca2+ ostéoporose : biphosphonates T score ≤ 1.5 : biphosphonates ? Traiter même après fracture
CONCLUSIONS (2) PREVENTION+++ TABAC+++ C’est aussi mauvais pour l’os !!!!! NUTRITION (calcium, vit D) POIDS NORMAL EXERCICE PHYSIQUE ALCOOL, CAFEINE HORMONOTHERAPIE LIMITATION DOSE, DUREE CORTCOIDES MEILLEURE CONTRÔLE DE LA MALADIE SURVEILLER SA TAILLE, DOULEUR