Download
1 / 59
600 likes | 1.07k Views
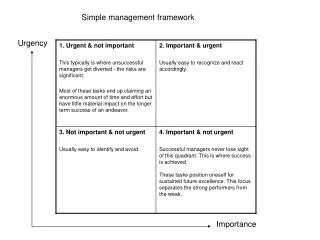
Urgency Frequency Syndrome. Hann-Chorng Kuo Department of Urology Buddhist Tzu Chi General Hospital Hualien. Lower Urinary Tract Symptoms. Storage symptoms -- Frequency, urgency, urge incontinence, nocturia, suprapubic pain Empty symptoms --

E N D
Urgency Frequency Syndrome Hann-Chorng Kuo Department of Urology Buddhist Tzu Chi General Hospital Hualien
Lower Urinary Tract Symptoms • Storage symptoms -- Frequency, urgency, urge incontinence, nocturia, suprapubic pain • Empty symptoms -- Hesitancy, intermittency, dysuria, poor stream, terminal dribble, residual sensation, micturition pain
The Urge Syndrome Sensory urgency – hypersensitivity of bladder or urethra or both, which causes -- a constant desire to void which is unrelieved by voiding -- a desire to void at a low bladder volume Motor urgency – occurrence of involuntary detrusor contractions which make patients urge to void and/or urine leakage
Frequency & Polyuria (Pollakisuria) • A number of patients may have large daily urine output >2800ml/day • Polydipsia, high water intake • Frequency with voided volume >350ml is physiologically normal • Should check metabolic status (DM, azotemia, hyperlipidemia, etc.) or diuretics
Sensory Urgency & Frequency • Reduced capacity of first desire (<150mL) or urgency (<350mL) subjectively • Absence of detrusor instability • Absence of urinary tract infection • The incidence of sensory urgency has been estimated 6%, compared with an incidence of 31% for detrusor instability
Known Causes of Sensory urgency freqency • Urinary tract infection • Lower ureteral stone or bladder stone • Bladder tumor • Irradiation cystitis • Interstitial cystitis • Chonic cystitis and reduced capacity • Foreign body or bladder injury
Etiology of Idiopathic Urgency Frequency • Psychological factors • Urothelial leak syndrome • Reduced bladder compliance • Diuresis • Learned habit • Detrusor instability • Occult neuropathy
Sensory UrgencyA Psychosomatic Complaint ? • Bladder retraining is effective in treating sensory urgency • Relaxation training, biofeedback, hypnosis, acupuncture have a 85% initial response, but relapse rate is 50% • Cognitive factor to maintain high stress and arousal levels, increase vigilance concerning bladder sensation and fullness
Psychological Social & Psychiatrical Factors • High level of distress • High level of anxiety • Symptoms may worsen in relation to work or stress • Belief of relationship with disease – uremia, infection, cancer • Overestimate the significance of symptoms
Sensory Urgency Frequency • A disease of exclusion • Acute symptoms and chronic symptoms? • Related to empty symptoms or not? • Related to painful syndrome (painful bladder, painful perineum, urethral pain)? • Intermittent? Persistent? Waxing & waning? • Related to urge or stress incontinence?
Diagnostic Work-up • Urinalysis • Uroflowmetry & residual urine amount • Voiding diary – 3 days • KUB or Cystoscopy • Ultrasound of bladder and urethra • Cystometry & sphincter EMG • Pressure flow study or videourodynamics
Pathophysiology of LUTS in 256 Taiwanese Women • Normal bladder and urethra 46 • Hypersensitive bladder 102 • Detrusor instability 44 • Low detrusor contractility 77 • Poor relaxation of urethral sphincter 76 • Genuine stress urinary incontinence 49 • Bladder outlet obstruction 21
Urethral sensitivityAn etiology of urgency frequency? • Increased urethral sensitivity was found in reduced bladder capacity and in women with normal CMG who complain of frequency urgency & dysuria • A higher incidence of bladder neck incompetence in patients with urgency frequency than the controls • Pelvic floor exercises and bladder neck suspension improves urgency frequency symptoms
Ultrasound of Bladder neck incompetence in urgency frequency
Bladder Neck Decsent & Incompetence before Pelvic Floor exercises
Improved Bladder neck Incompetence after Pelvic Floor exercises
Detrusor Instability as an etiology of urgency frequency • Minute detrusor contraction occur in the normal bladder – C-fiber dominates? • Increased perception of bladder fullness during diuresis • No significant difference in perception of bladder fullness between sensory urgency and detrusor instability • Similar clinical efficacy of oxybutynin in treating sensory urgency (62.5%) and DI (60.4%)
Increased amplitude of detrusor contractions in bladder filling
Sensory nerves of bladder • Dual sensory innervation of mammalian bladder • Myelinated A-delta fibers – mediate stretch and micturition reflex • Unmyelinated C-fibers (capsaicin sensitive sensory fibers) – mediate pain, temperature, noxious stimuli • Sensory axons are present in lamina propria
Capsaicin sensitive sensory fiber • Sensory function – regulating micturition threshold (especially after spinal cord transection), mediating pain, activating cardiovascular responses • Efferent function – activating local motor responses, regulating nerve excitability, local control of vascular blood flow and permeability (neurogenic inflammation ?)
Treatment of sensory urgency by intravesical capsaicin • Capsaicin in 10 micro-M can effectively treat hypersensitive disorders • Transient desensitization of capsaicin-sensitive afferents without interfering motor function • Little effect was found in classical Interstitial cystitis • Resiniferatoxin may have similar effects
Role of Potassium in pathogenesis of Urgency Frequency Syndrome • Chronic diffusion of urinary potassium into bladder interstitium may induce sensory symptoms, damage tissue, and possibly cause interstitial cystitis • Intravesical potassium test (40ml, 0.4M) is a reliable method for detecting abnormal urothelium permeability
Nerve Growth Factor • Increased nerve growth factor levels in the bladder biopsies from sensory urgency, chronic cystitis, and interstitial cystitis than in controls • Immunostaining showed increased NGF expression in the urothelium, most marked in idiopathic sensory urgency • Anti-NGF treatment may be rational
Urgency frequency associated with Bladder or perineal pain • Suprapubic pain or perineal pain at bladder fullness • The pain may/not disappear after voiding • A tight sphincter EMG at bladder capacity • Reduced bladder compliance • Urethral obstruction due to stricture or spastic urethral sphincter as etiologies
Differential diagnosis of Urgency Frequency Syndrome • History – Bladder injury, foreign body • Urinalysis – UTI • Uroflowmetry – BOO • Cystoscopy – bladder tumor, bladder stone, irradiation cystitis, chronic cystitis • Ultrasound – bladder neck and/or urethral incompetence • Cystometry – low compliance, DI, DESD
Pressure flow study for Urgency frequency syndrome • Cystometry can only detect capacity, detrusor instability, compliance, and bladder sensation during filling phase • Pressure flow study can diagnose bladder outlet obstruction, low detrusor contractility, poor relaxation of urethral sphincter, and DESD accurately
Urodynamic study in Urgency frequency syndrome- Detrusor overactivity
Urodynamic study in Urgency frequency syndrome- Detrusor underactivity
Urodynamic study in Urgency frequency syndrome- Bladder outlet obstruction
Urodynamic study in Urgency frequency syndrome- Low compliant bladder
Urodynamic study in Urgency frequency syndrome- Pseudodyssynergia
Urodynamic study in Urgency frequency syndrome- Idiopathic Sensory Urgency
Treatment of Frequency urgency syndrome & Normal UDS • Reassurance • Bladder biofeedback • Restrict fluid intake • Avoid diuretics and certain acid foods • Sedatives or mild tranquilizers
Bladder biofeedback for Urgency frequency syndrome • Urodynamic proven sensory urgency • Bladder biofeedback – increased each voiding interval by holding urine for 5 min more • Increase fluid intake gradually • Improved functional capacity (296 v 96ml) and decreased daytime frequency (5.7 v 15.8) and nocturia (0.3 v 2.3) after treatment
Intravesical Heparin therapy • Patients with urgency frequency and a positive potassium test • Intravesical Heparin 25000u/10ml saline and holding for 2 hours • 2x or 3x per week for 12 weeks • 67% patients have improvement in symptoms and increase in bladder capacity
The changes of urodynamic parameters before and after heparin treatment
Intravesical Capsaicin Therapy • Patients who are refractory to conventional treatment • Capsaicin 10 -5 M in 30ml N/S instilled to bladder for 30 minutes • Resiniferatoxin 10-8 M in 30ml N/S • A burning sensation or urge at instillation • Relief of pain and urge in the later days
A Cocktail Preparation for Idiopathic Urgency Frequency ? • Mixture of Xylocaine, Resiniferatoxin, Heparin, Oxybutynin with certain vehicle • To provide local anesthesia, C-fiber desensitization, repair of defected glycosaminoglycan layer, anticholinergic effect together in one instillation • Clinical trial is undergoing
Anticholinergics Treatment • Oxybutynin – the most effective and safe drug currently available • Detrusitol – M3 antagonist, less salivary and GI side effects than ditropan • Flavoxate – mild effect in detrusor • Imipramine – central and anticholinergics