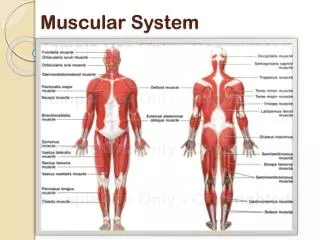
Muscular System
Muscular System. As with the skeltal system most of the muscular system also develops from the mesodermal germ layer Smooth muscle develops from splanchnic mesoderm which surrounds gut /derivatives. • Cardiac muscle develops from splanchnic mesoderm which surrounds the heart tube.

Muscular System
E N D
Presentation Transcript
Muscular System • As with the skeltal system most of the • muscular system also develops from the • mesodermal germ layer • Smooth muscle develops from splanchnic • mesoderm which surrounds gut /derivatives. • • Cardiac muscle develops from splanchnic • mesoderm which surrounds the heart tube.
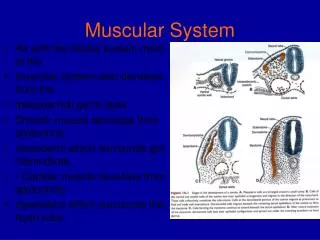
TRUNK MUSCULATURE • Skeletal muscle of the • trunk develops from • paraxial mesoderm • (which forms somites & • somitomeres) • • Somites differentiate
Somites differentiate • into:- • 1. Sclerotome → Axial • skeleton & • 2. Dermomyotome → • a.Dermatome dermis • and subcut tissues & b. • Myotome segmental • muscles (& takes with it • its own segmental nerve).
FATE OF MYOTOME CELLS • Myotome cells split • off, move to their • definitive locations, & • become elongated & • spindle shaped • (called myoblasts) • Many myoblasts fuse • to become • Multinucleated muscle fibres.
Myofibrils appear in • cytoplasm. • By 12/52 cross • striations typical for • skeletal muscle • appear.
Somites: form body wall musculature. It forms a dorsal epimere & a • ventral hypomere. • The epimere forms the vertebral extensors; while the hypomere forms • the muscles of the body wall and limbs. • Note the different innervation viz. dorsal and ventral primary rami
Somitomeres • same process in head and neck region i.e. form myoblasts which will form extra ocular eye muscles, face, larynx, tongue etc
Limb Musculature • Condensation of mesenchyme near the base of limb buds (7th week) • Mesenchyme is derived from dorsolateral cells of somites • Migrate into limb bud to form the muscles • Connective tissue dictates the pattern of muscle formation • Upper limb buds lie opposite the lower five cervical and upper two thoracic segments
Limb Musculature • Lower limb buds lie opposite lower foua lumbar and upper two sacral segments • There is a 180° medial rotation of the lower limb compared to developing upper limb (angle of flexion differs)
Cardiac Muscle • Develops from splanchnic mesoderm surrounding the endothelial heart tube • Myoblasts adhere to one another by intercalated discs • Myofibrils develop as in skeletal muscle but do not fuse • Few special bundles become visible (Purkinje fibers)
INTRAEMBRYONIC COELOM • Appears as isolated spaces in the lateral mesoderm • In the 4th week, the spaces fuse to form a single horseshoe-shaped (U-shaped) cavity • The coelom divides the lateral mesoderm into: • Somatic (parietal) layer: under ectoderm • Splanchnic (visceral) layer: over endoderm
Somatopleure = somatic mesoderm + overlying ectoderm • Splanchnopleure =splanchnic mesoderm + underlying endoderm
DERIVATIVES: It gives rise to three body cavities: • A pericardial cavity: the curve of U • Two pericardioperitoneal canals (future pleural cavities): the proximal parts of the limbs of U • Two peritoneal cavities: the distal parts of the limbs of U • Each cavity has a parietal layer (derived from somatic mesoderm) & a visceral layer (derived from visceral mesoderm) • FUNCTION: It provides space for the organs to develop & move
DEVELOPMENT OF PERITONEAL CAVITY • Major part of intraembryonic coelom • Develop from the distal parts of the limbs of the U-shaped cavity • Originally, it is connected with extraembryonic coelom (midgut herniates to the outside through this connection) • At 10th week, it looses its connection with extraembryonic ceolom (when midgut returns to abdomen)
DEVELOPMENT OF PERITONEAL CAVITY • Originally, there were 2 peritoneal cavities • After lateral folding of embryo, the peritoneum becomes a single cavity HOW?
MESENTERIES • A MESENTERY is a double layer of peritoneum that begins as an extension of the visceral peritoneum covering an organ • The mesentery connects the organ to the body wall and transmits vessels and nerves to it • Transiently, the dorsal & ventral mesenteries divide the peritoneal cavity into right & left halves • The ventral mesentery disappears EXCEPT where stomach develops • (WHY?)
PERICARDIAL CAVITY • Develops from the curve of the U-shaped cavity • During formation of head fold, the heart & pericardial cavity move ventrocaudally & become anterior to the foregut (esophagus) • It is bounded by an outer somatic & an inner visceral layer, forming the serous pericardium
PERICARDIAL CAVITY • Originally, it is connected with the 2 pericardioperitoneal canals • Later on, it become separated from the 2 pericardioperitoneal canals HOW?
PERICARDIAL CAVITY • Originally, the bronchial buds are small relative to the heart • Bronchial buds grow laterally into pericardioperitoneal canals (future pleural cavities) • Pleural cavities expand ventrally around heart & splits mesoderm into: • Outer layer: forms thoracic wall • Inner layer:pleuropericardial membrane
PLEUROPERICARDIAL MEMBRANES • THE PARTS SURROUNDING THE SEROUS PERICARDIUM: form the fibrous pericardium • THE PARTS BEHIND THE HEART: fuse with the ventral mesentery of the esophagus (at 7th week), forming the mediastinum & separating pericardial from pleural cavities • N.B.: The right pleural cavity separates from pericardial cavity earlier than left
PLEURAL CAVITIES • Develop from the 2 pericardiperitoneal canals • Originally, they are connected with pericardial & peritoneal cavities • Later on, they become separated from: • Pericardial cavity • Peritoneal cavity (HOW?)
PLEUROPERITONEAL MEMBRANES • Produced when developing lungs & pleural cavities expand into the body wall • During 6th week, they fuse with dorsal mesentery of esophagus & septum transversum, separating pleural cavities from peritoneal cavity • N.B.: The right pleural cavity separates from peritoneal cavity earlier than left
DEVELOPMENT OF DIAPHRAGM • The diaphragm develops from: • Septum transversum: forms the central tendon • Dorsal mesentery of esophagus: forms the right & left crus • Muscular ingrowth from lateral body wall:posterolateral part (costal part) • Pleuroperitoneal membranes: small portion of diaphragm
SEPTUM TRANSVERSUM • At 3rd week, it is in the form of mass of mesodermal tissue in the cranial part of embryo (opposite the 3rd, 4th & 5th cervical somites) • At 4th week (during formation of head fold), it moves ventrocaudally forming a thick incomplete partition between thoracic & abdominal cavities • At 6th week, it expands & fuse with dorsal mesentery of esophagus & pleuroperitoneal membranes to form the diaphragm
INNERVATION OF DIAPHRAGM • Myoblasts from 3rd, 4th & 5th cervical somites migrate into diaphragm & bring their nerve fibers from them • Nerve fibers derived from ventral rami of 3rd, 4th & 5th cervical nerves fuse to form phrenic nerve that elongate to follow the descent of diaphragm • Both motor & sensory supply of the diaphragm is derived from phrenic nerve • The part of diaphragm derived from lateral body wall receives sensory fibers from lower intercostal nerves
ANOMALIES OF DIAPHRAGM • CONGENITAL DIAPHRAGMATIC HERNIA • EVENTRATION OF DIAPHRAGM • CONGENITAL HIATAL HERNIA
CONGENITAL DIAPHRAGMATIC HERNIA • A posterolateral defect of diaphragm • Cause: defective formation and/or fusion of pleuroperitoneal membrane with other parts of diaphragm • Effects: • Herniation of abdominal contents into thoracic cavity • Peritoneal & pleural cavities are connected with one another • The defect usually occurs in the left side (WHY?)
EVENTRATION OF DIAPHRAGM • Cause: failure of muscular tissue from body wall to extend into pleuroperitoneal membrane on one side • Effects: superior displacement of abdominal viscera (surrounded by a part of diaphragm forming a pocket)
CONGENITAL HIATAL HERNIA • Herniation of part of the stomach through a large esophageal hiatus (opening)
Reference • clanatomy.ukzn.ac.za/...Embryology/EMBRYOLOGY_OF_MUSCULAR • HENRY Gray 1821-1865 anatomy of the human body. • http://www.youtube.com/watch?v=8VFAF_piggl