Download
1 / 16
330 likes | 1.16k Views
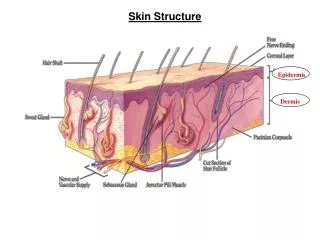
Structure of the Skin. The largest organ of the body. Its surface area is responsible for the regulation of body temperature Has three layers

E N D
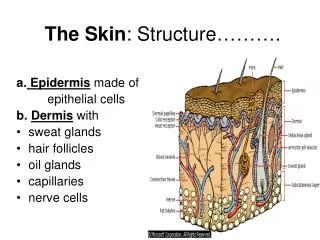
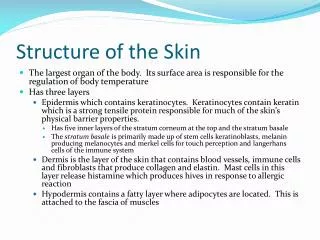
Structure of the Skin • The largest organ of the body. Its surface area is responsible for the regulation of body temperature • Has three layers • Epidermis which contains keratinocytes. Keratinocytes contain keratin which is a strong tensile protein responsible for much of the skin’s physical barrier properties. • Has five inner layers of the stratum corneum at the top and the stratum basale • The stratum basale is primarily made up of stem cells keratinoblasts, melanin producing melanocytes and merkel cells for touch perception and langerhans cells of the immune system • Dermis is the layer of the skin that contains blood vessels, immune cells and fibroblasts that produce collagen and elastin. Mast cells in this layer release histamine which produces hives in response to allergic reaction • Hypodermis contains a fatty layer where adipocytes are located. This is attached to the fascia of muscles
Picture courtesy of : http://www.best-anti-aging-guide.com/images/human-skin.jpg
Rapidly dividing stem cell keratinocytes in the basal layer grow and divide in this layer • As the days pass the mitotic cells migrate into the upper layers of the epidermis dehydrate and begin to degenerate • By the time the keratinocytes arrive at the stratum corneum they are dead and the keratin protein becomes hardened and resistant to the environment and most chemical insults • In the average person this migration of cells from the basale layer to the stratum corneum occurs every 30 days. • In diseases like psoriasis this turnover rate is dramatic increase to as little as 72 hours producing scaly skin
Functions of the skin • Provides a physical barrier to infections • Provides a barrier to the lose of water • Temperature regulation via sweating • Enable the sense of touch • Vitamin D is synthesized from cholesterol
Immune function of skin • The skin is not a sterile environment. On the skin, bacteria and fungi are present. • The normal flora of the skin provides a competitive environment that protects against invasion by more pathogenic organisms • Skin contains immune system cells including lymphocytes (small degree), mast cells, and dendritic cells • Mast cells contain histamine and when the mast cells meet an antigen they release histamine to produce a “wheal and flare” reaction • Dendritic cells capture and process antigens, these cells carry the “invader” to regional lymph node to initiate a possible immune reaction
Medical terminology involving the skin • Macule: flat pigmented lesion • Papule: Slightly raised lesion (<5 mm) (pimple) • Maculopapular: combination of the two usually the papule is in the center of the macule. Sometimes called morbilliform (“measle like”) • Erythema: beffy red section of skin • Plaque: raised area of skin with clear borders. • Nodule : a raised lesion (> 5mm) • Vesicle: a small raised lesion filled with clear fluid(Blister) • Bulla: a large raised lesion filled with clear fluid • Pustule: a raised lesion filled with pus and bacterially infected fluids
Diseases of the skin • Autoimmune diseases of the skin • Psoriasis. In psoriasis the immune system of the body attacks the cells of the upper layers of the skin. The patient develops rashes, intense erythema that leads to scales and blisters localized to plaques areas. Can be painful • T cells enter the epidermis and attack the keratinocytes of the skin which produce chronic inflammation • Drugs that suppress the immune system are used • Topical steroid preparations: Desoximetasone (Topicort®), Fluocinolide (lidex®). • Coal Tar agents: Anthralin cream (Psoriatec®) • Topical immune system medications: Pimecrolimus (Elidel®) • Vitamin D derivatives: Calcipotriene (Dovonex®)
If topical therapy fails then internal therapy can be tried: • Methotrexate: 5-25 mg PO weekly • Cyclosporin (Neoral ®, Sandimmune®, Gengraf ®): 5 mg/kg daily • Mycophenolate (Cellcept®):250-500 mg/day • All these agents are agents that suppress the immune system
ATOPIC DERMATTIS (ECZEMA) • Eczema is similar to psoriasis but less severe • Eczema is believed to be a hereditary allergic reaction of the skin to a normally benign antigen(s) • Eczema is sometimes called “atopic dermatitis” and is commonly associated with asthmatic patients • Affected areas are itchy, red, and warm to the touch. Lesions may enlarge and become scaly. The rash are very itchy and the scratching can damage the skin further. • Treatment includes: • Topical Steroids • Vitamin D derivatives (Dovonex) • Vitamin A derivatives (retinoids): Differin® (Adapalene) • Topical immune modulators: Pimecrolimus (Elidel®)
Acne • Inflammatory reaction in the skin called by excessive production of sebum in the sebaceous glands of the skin located near hair follicles. • Bacteria known as Propriobacterium acnes feeds on the fats and release fatty acids which causes the skin to become inflammed • A severe form of acne is nodulocystic acne which can form life long scars • Therapy: • Benzoyl Peroxide (Oxy 10, Brevoxyl®, Acne 10®) • Topical antibiotics combined with benzoyl peroxide i.e Benzaclin ® is Clindamycin and benzoyl peroxide • Topical Vitamin A derivatives: Retin A® (tretinoin ) • Oral Contraceptive in females: Ortho Tri Cyclen® • Nodulocytic acne: Accutane ® (isotretinoin) A oral medication. • Must be registered in the FDA’s iPLEDGE system
Bacterial Infections • Most commonly seen infections are impetigo in children and folliculitis in adults • Both are caused by staphylococcal infections • Cured by penicillin type antibiotics: • Dicloxacillin 500 mg capule three times a day for 10 days
Viral Infections • Chicken Pox: Varicella Zoster Virus is the cause. Highly contagious by either touch or airborne sneezing. No medication really effective, sometimes acyclovir is tried in immunosuppressed patients. Calamine lotion® is effective in suppressing itch and crusting the lesions. • Measles: very contagious. caused by the respiratory virus Rubeola (not really a skin disease but has skin manifestation) • Shingles: Varicella Zoster virus is the cause. If this is seen in young patients it can mean HIV infection
Cancers of the skin • Any skin lesion that is large, raised, asymmetric, changes in color, and has raggy edges should raise the suspicion of cancer • Malignant melanoma is a cancer of the pigment producing cells of the skin and can be fatal if allowed to spread to other areas of the body • Basal Cell Carcinoma is a serious cancer; however, it can be cured with chemotherapy
Miscellaneous disorders of the skin • Wrinkles are caused by a lack of elastin in the skin and reduce sebum production. It is common in old age and sun exposed skin • Rosacea is also known as “adult” acne. Its cause is not known • Burns • Decibutus ulcers
Skin manifestations to drug • Skin is often the window to seeing an incipient drug allergy • Intense itching, wheals, hives may indicate an Type 1 hypersensitivity to a drug (anaphylactic reaction) • Penicillins and other beta lactams • Sulfa drug • Antiseizure drugs (Carbamazepine) • Upon subsequent exposure a life threatening reaction can occur • Morbilliform reaction: Type 4 hypersensitivity to a drug. Usually occurs with 72 hours after drug exposure • Usually not life threatening but uncomfortable to the patient
Stevens Johnson Syndrome and Toxic Epidermal Necrolysis • A drug reaction involving CD8 lymphocytes and epidermal antigens and the drug • SJS and TEN represent a dermatological emergency • The reaction involves confluent separation of the epidermis from the dermis and a denuding of the skin • Therapy involves that used for severe third degree burns • IV Corticosteroids is controversial • IVIG 2 gm IV X1 or 0.4 g /day X 5 days has being tried with some success. • Common drug precipants: Penicillins, Sulfasalazine, phenytoin, lamotrigine, Levetiractam , allopurinol, phenobarbital, ibuprofen http://www.youtube.com/watch?v=BC-OLAoqCk4