Ebola Facts
260 likes | 418 Views
Ebola Facts. Symptoms, Diagnosis, Treatments, Protection, Preparedness. Updated 10/21/14. Symptoms of Ebola. Initial symptoms are nonspecific - may include fever, chills, myalgias, and malaise. Patients can progress to develop gastrointestinal symptoms:

Ebola Facts
E N D
Presentation Transcript
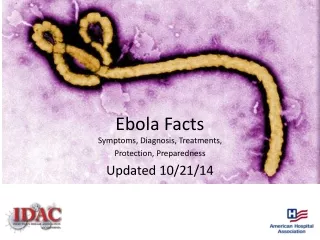
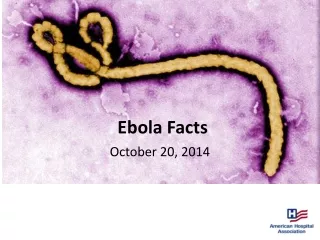
Ebola Facts Symptoms, Diagnosis, Treatments, Protection, Preparedness Updated 10/21/14
Symptoms of Ebola • Initial symptoms are nonspecific - may include fever, chills, myalgias, and malaise. • Patients can progress to develop gastrointestinal symptoms: • severe watery diarrhea, nausea, vomiting, abdominal pain • Other symptoms: • chest pain, shortness of breath, headache or confusion, conjunctival injection, hiccups, seizures, and cerebral edema • Bleeding not universally present but can manifest later as petechiae, ecchymosis/ bruising, or oozing. Frank hemorrhage less common. • Some develop diffuse erythematous maculopapular rash that can desquamate. • Most common symptoms reported during current outbreak: • fever (87%) • fatigue (76%) • vomiting (68%) • diarrhea (66%) • loss of appetite (65%) • Patients with fatal disease develop more severe clinical signs early during infection and die between days 6 - 16 of complications (mean of 7.5 days). • In non-fatal cases, patients may have fever for several days and improve, around day 6. • The case fatality proportion in West Africa is about 71% Source: Centers for Disease Control and Prevention. http://www.cdc.gov/vhf/ebola/hcp/clinician-information-us-healthcare-settings.html Accessed Oct. 14, 2014
Diagnosis of Ebola • Diagnosing Ebola can be difficult at first since early symptoms, such as fever, are nonspecific to Ebola infection. • However, if a person has the early symptoms and has had contact with Ebola they should be isolated and public health professionals notified. • Samples from the patient can then be collected and tested to confirm infection. Source: Centers for Disease Control and Prevention http://www.cdc.gov/vhf/ebola/diagnosis/index.html Accessed Oct. 14, 2014
Source: http://www.cdc.gov/vhf/ebola/pdf/checklist-patients-evaluated-us-evd.pdf Accessed Oct. 14, 2014
Clinical Progression of Ebola Source: Jonathan B. Perlin, MD, PhD and HCA Clinical Excellence Knowledge Center, 2014
Treatment of Ebola • There are no approved treatments available for EVD. • Clinical management focus - supportive care of complications: • hypovolemia, electrolyte abnormalities, hematologic abnormalities, refractory shock, hypoxia, hemorrhage, septic shock, multi-organ failure, and DIC. • Recommended care includes: • volume repletion • maintenance of blood pressure (with vasopressors if needed) • maintenance of oxygenation • pain control • nutritional support • treating secondary bacterial infections and pre-existing comorbidities • Among patients from West Africa, large volumes of intravenous fluids have often been required to correct dehydration due to diarrhea and vomiting. • Several investigational therapeutics for Ebola virus disease are in development. There are no approved vaccines available for EVD. Several investigational Ebola vaccines are in development, and Phase I trials are underway for some vaccine candidates. Source: Centers for Disease Control and Prevention. http://www.cdc.gov/vhf/ebola/hcp/clinician-information-us-healthcare-settings.html Accessed Oct. 14, 2014
Clinical Evidence Source: Jonathan B. Perlin, MD, PhD and HCA Management Services, L.P. 2014
Clinical Evidence Source: Jonathan B. Perlin, MD, PhD and HCA Management Services, L.P. 2014
Clinical Evidence Source: Jonathan B. Perlin, MD, PhD and HCA Management Services, L.P. 2014
Revised Guidance on PPE for Health Care Workers • Updated guidance on PPE to be used and processes for donning and doffing PPE for health care workers entering a patient room hospitalized with Ebola. Emphasizes the importance of training, practice, competence, and observation of health care workers in correct donning and doffing of PPE selected by the facility. • Key principles: • Prior to patient contact, all workers must have repeated training and demonstrated competency in Ebola-related infection control, and specifically donning/ doffing proper PPE. • While working in PPE no skin should be exposed. • Overall safe care must be overseen by onsite manager at all times, and each step of every PPE donning/doffing procedure supervised by a trained observer • Ebola is spread through direct contact with blood or body fluids or with contaminated objects. For all workers, full body coverage PPE is recommended to reduce the risk of self-contamination • To protect workers, facilities must provide onsite management and oversight on safe use of PPE and implement administrative and environmental controls Source: Centers for Disease Control and Prevention. This guidance is current as of October 20, 2014 from http://www.cdc.gov/vhf/ebola/hcp/procedures-for-ppe.html. Please see website for complete details.
Recommended Administrative and Environmental Controls for Healthcare Facilities • Protecting workers and preventing spread of Ebola requires proper administrative procedures and safe work practices including : • Implement triage protocols to identify potential patients and institute precautions • Designate site managers overseeing implementation of safety precautions: • Site managers monitor supply and evaluate care in isolation area • At least one site manager always on-site where Ebola patient is being treated • Identify ahead of time critical care functions and essential workers: • For Ebola patient care • For collection of laboratory specimens • For environmental management and waste • Ensure workers are trained in all recommended protocols and PPE • Workers should practice donning/doffing procedures and demonstrate competency during training before caring for patients • Use trained observers to monitor correct PPE use and protocol adherence and guide workers using a checklist for every donning /doffing procedure • Document observer and worker training in donning/doffing and performing necessary care-related duties while wearing PPE • Designate spaces so that PPE can be donned and doffed in separate areas Source: Centers for Disease Control and Prevention. This guidance is current as of October 20, 2014 from http://www.cdc.gov/vhf/ebola/hcp/procedures-for-ppe.html. Please see website for complete details.
Recommended Administrative and Environmental Controls for Healthcare Facilities • Key safe work practices include: • Isolate patient in room with closed door and private bathroom as soon as possible. • Limit contact with patient and restrict non-essential personnel and visitors. • Monitor patient care area and log entry and exit of all workers • Ensure trained observer watches each donning and doffing procedure and provides supervisory assurance • Ensure workers have sufficient time to don and doff PPE correctly • Ensure practical precautions taken during patient care: • keeping hands away from the face • limiting touch of surfaces and body fluids • preventing needlestick and sharps injuries • performing frequent disinfection of gloved hands using an alcohol-based hand rub • Disinfect visibly contaminated PPE, surfaces, or equipment • Perform regular cleaning and disinfection of patient care area surfaces • Performed by nurses or physicians as part of patient care activities to limit workers in room. • Implement worker observation in the patient room, if possible • Establish exposure management plan that addresses decontamination and follow-up of an affected worker. Training on plan and follow-up should be part of the worker training. Source: Centers for Disease Control and Prevention. This guidance is current as of October 20, 2014 from http://www.cdc.gov/vhf/ebola/hcp/procedures-for-ppe.html. Please see website for complete details.
Recommended PPE • Key to all PPE is consistent implementation through repeated training and practice. • Facility should select and standardize PPE for all essential workers directly interacting with Ebola patients • Provide written protocol outlining procedures for donning and doffing of PPE, and review and monitor by trained observer • CDC recommends facilities use a powered air-purifying respirator (PAPR) or an N95 or higher respirator in the event of an unexpected aerosol-generating procedure. • For healthcare workers who spend extended periods in PPE, safety and comfort are critical. Standardizing attire under PPE (e.g., surgical scrubs or disposable garments and dedicated washable footwear) facilitates donning and doffing process and eliminates concerns of contamination of personal clothing. • If facilities elect to use different PPE from what is outlined by CDC (e.g., coveralls with either an integrated hood or a surgical hood with integrated full face shield), they must train workers and ensure that donning and doffing procedures are adjusted and practiced accordingly. Source: Centers for Disease Control and Prevention. This guidance is current as of October 20, 2014 from http://www.cdc.gov/vhf/ebola/hcp/procedures-for-ppe.html. Please see website for complete details.
Recommended PPE • PAPR or N95 Respirator • PAPR: A PAPR with a full face shield, helmet, or headpiece. Any reusable helmet or headpiece must be covered with a single-use (disposable) hood that extends to shoulders and fully covers neck and is compatible with selected PAPR. • A PAPR with a self-contained filter and blower unit integrated inside the helmet is preferred. • A PAPR with external belt-mounted blower unit requires adjustment of the sequence for donning and doffing. • N95 Respirator: Single-use (disposable) N95 respirator in combination with single-use (disposable) surgical hood extending to shoulders and single-use (disposable) full face shield. If N95 respirators are used instead of PAPRs, careful observation is required to ensure workers are not inadvertently touching faces under face shield during care. • Single-use (disposable) fluid-resistant or impermeable gown that extends to at least mid-calf or coverall without integrated hood. Coveralls with or without integrated socks are acceptable. Consideration should be given to gowns or coveralls with thumb hooks to secure sleeves over inner glove. • Single-use (disposable) nitrile examination gloves with extended cuffs. Two pairs of gloves should be worn. At a minimum, outer gloves should have extended cuffs. • Single-use (disposable), fluid-resistant or impermeable boot covers that extend to at least mid-calf or single-use (disposable) shoe covers. Boot and shoe covers should allow for ease of movement and not present a slip hazard to the worker. • Single-use (disposable) fluid-resistant or impermeable shoe covers are acceptable only if they will be used in combination with a coverall with integrated socks. • Single-use (disposable), fluid-resistant or impermeable apron that covers torso to level of mid-calf should be used if Ebola patients have vomiting or diarrhea. If a PAPR will be worn, consider selecting an apron that ties behind the neck to facilitate easier removal during the doffing procedure. Source: Centers for Disease Control and Prevention. This guidance is current as of October 20, 2014 from http://www.cdc.gov/vhf/ebola/hcp/procedures-for-ppe.html. Please see website for complete details.
For more detail on PPE for Health Care Workers, please visit: http://www.cdc.gov/vhf/ebola/hcp/infection-prevention-and-control-recommendations.html Source: http://www.cdc.gov/vhf/ebola/pdf/ppe-poster.pdf Accessed Oct. 14, 2014
External (Non-CDC) Resources on PPE • Emory Healthcare: Ebola Preparedness Protocols • University of Nebraska Medical Center: PPE for Ebola • Médecins Sans Frontières (Doctors without Borders): Filovirus Haemorrhagic Fever Guideline, 2008[PDF - 134pages] • World Health Organization (WHO): Infection prevention and control guidance for care of patients in health-care settings, with focus on Ebola Source: Centers for Disease Control and Prevention. Accessed October 20, 2014 from http://www.cdc.gov/vhf/ebola/hcp/procedures-for-ppe.html
Hospital Preparedness Checklist • Every hospital should ensure that it can detect a patient with Ebola, protect health care workers, and respond in a coordinated fashion. • Many signs and symptoms of Ebola are non-specific and similar to common diseases. • Transmission can be prevented with appropriate infection control measures. • Checklist highlights key areas for hospital emergency management officers, infection control practitioners, and clinicians to detect possible Ebola cases, protect employees, and respond appropriately. • Hospitals should review infection control procedures and incorporate plans for administrative, environmental, and communication measures, as well as personal protective equipment (PPE) training and education. • Hospitals should also define the individual work practices that will be required to detect the introduction of a patient with Ebola, prevent spread, and manage the impact on patients, the hospital, and staff. Source: Centers for Disease Control and Prevention;. Accessed October 15, 2014 http://www.cdc.gov/vhf/ebola/pdf/hospital-checklist-ebola-preparedness.pdf
Hospital Preparedness Checklist • Detect: • Screen patients for symptoms and risk factors for Ebola, including fever of greater than 101.5 degrees and travel to West Africa (in particular, Guinea, Liberia and Sierra Leone). • Patients meeting criteria should be immediately isolated and tested. • Conduct periodic checks to confirm screening procedures and notification, isolation and personal protective equipment (PPE) procedures. • Protect: • Use CDC-recommended infection control practices • Review, implement and drill with first-contact personnel, clinicians, ancillary staff, and others as appropriate on: • Infectious disease procedures and protocols • Triage techniques and Ebola screening questions • Disease identification, testing, specimen collection and transport procedures • Isolation, quarantine and security procedures • Communications and reporting procedures • Cleaning and disinfection procedures • Respond: • All staff should know what to do when encountering a suspected Ebola patient. • Ebola is a nationally notifiable disease and must be reported to public health authorities. • Ensure hospital is in contact with local/state health department to confirm communication strategies. • Review plans and protocols, and exercise/test ability to share relevant health data. Source: American Hospital Association, adapted from Centers for Disease Control and Prevention Detailed Hospital Checklist for Ebola Preparedness. http://www.cdc.gov/vhf/ebola/pdf/hospital-checklist-ebola-preparedness.pdf Accessed October 15, 2014
Surgical Protocol for Possible or Confirmed Ebola Cases • Elective surgical procedures should not be performed in cases of suspected or confirmed Ebola. • In cases where an emergency operation must be performed this protocol should be implemented to minimize risk to hospital personnel. • The choice of operative approach (open or MIS) should take into consideration minimizing potential hazards to all members of the OR team. • Although protocols for Personal Protective Equipment (PPE) are in place, there is no guideline for operating room personnel and surgical providers. • The American College of Surgeons has adapted Centers for Disease Control and Prevention recommendations to the OR environment. Source: American College of Surgeons. https://www.facs.org/ebola/surgical-protocol Updated October 6, 2014. Accessed October 16, 2014
Surgical Protocol - Possible or Confirmed Ebola Cases • Patient Transport and Transfer to OR • Health care providers should wear the following to transport and transfer a patient to OR. • Gloves • Level 3 AAMI fluid resistant gown • eye protection (goggles or face shield) • Facemask • Surgical Checklist • Ebola status discussed in pre- and post-op briefing as integral part of Safe Surgery Checklist • All personnel should be aware of potential risks of exposure • OR Staff Personal Protection Equipment • Due to significant risk of exposure all OR room personnel should wear: • Personal Protective Gear • AAMI Level 4* Impervious Surgical Gowns • Leg coverings with full plastic film coating over fabric not just over foot area • Full face shield • Mask • Double gloves • Surgical hood • *Level 4 AAMI rated gowns, drapes, and protective apparel demonstrate the ability to resist liquid and viral penetration in a laboratory test, ASTM F1671. Source: American College of Surgeons. https://www.facs.org/ebola/surgical-protocol, Updated Oct. 6, 2014. Accessed October 16, 2014
Surgical Protocol - Possible or Confirmed Ebola Cases • Surgical Drapes • AAMI Level 4* drapes should be used • Instrumentation and Sharps • Keep sharps to a minimum • Use instruments, rather than fingers, to grasp needles, retract tissue, and load/unload needles and scalpels • Give a verbal announcement when passing sharps • Avoid hand-to-hand passage of sharp instruments by using a basin or neutral zone that has been agreed upon at the case start • Use alternative cutting methods such as blunt electrocautery • Substitute endoscopic surgery for open surgery when possible • Use round-tipped scalpel blades instead of pointed sharp-tipped blades • Use elctrocautery preferentially to scalpel for incisions • No needles or sharps on the Mayo stand • No recapping of needles • Use blunt tip suture needles when possible • Continue “sharps safety” techniques during OR table clean up post-procedure Source: American College of Surgeons. https://www.facs.org/ebola/surgical-protocol, Updated Oct. 6, 2014. Accessed October 16, 2014
Surgical Protocol - Possible or Confirmed Ebola Cases • 6. OR Staff Exposure • Persons with percutaneous or mucocutaneous exposures to blood, body fluids, secretions, or excretions should: • Stop working and immediately wash affected skin surfaces with soap and water • Mucous membranes (e.g., conjunctiva) should be irrigated with copious amounts of water or eyewash solution • Immediately contact hospital Infectious Disease consultant for post-exposure evaluation. • --------------------------------------------------------------------------------------------------------------------- • References • http://www.cdc.gov/hicpac/pdf/isolation/Isolation2007.pdf • http://www.cdc.gov/sharpssafety/resources.html • http://www.cdc.gov/vhf/ebola/hcp/infection-prevention-and-control-recommendations.html Source: American College of Surgeons. https://www.facs.org/ebola/surgical-protocol, Updated Oct. 6, 2014. Accessed October 16, 2014
References • Baize S. et al. Emergence of Zaire Ebola Virus Disease in Guinea - Prepminary Report. N Engl J Med. 2014 Apr 16. epub • Feldmann H , Geisbert TW. Ebola Haemorrhagic Fever. Lancet. 2011 Mar 5;377(9768):849-62. • Fowler RA, Fletcher T, Fischer WA, et al. Caring for Critically Ill Patients with Ebola Virus Disease: Perspectives from West Africa. Am J Respir Crit Care Med. 2014 Aug 25. Epub • Kortepeter MG, Bausch DG, Bray M. Basic Cpnical and Laboratory Features of Filoviral Hemorrhagic Fever. J Infect Dis. 2011 Nov;204 Suppl 3:S810-6 • WHO Ebola Response Team. Ebola Virus Disease in West Africa – The First 9 Months of the Epidemic and Forward Projections. N Eng J Med. 2014 Sept 23. Epub Source: http://www.cdc.gov/vhf/ebola/index.html Accessed Oct. 14, 2014
REFERENCES AND EVIDENCE CLASSIFICATION • Clinical management of patients with viral haemorrhagic fever: a pocket guide for the front-line health worker. World Health Organization. World Health Organization , 2014. April 2014. Level 3 • Ebola (Ebola Virus Disease). Centers for Disease Control and Prevention website http://www.cdc.gov/vhf/ebola/. Updated October 3, 2014. Accessed October 16, 2014. Level 3 • WHO finds 70 percent Ebola mortality rate. Aljazeera.com Aljazeera America, 15 Oct 2014. Web. 16 Oct 2014. • Ansari AA. Clinical features and pathobiology of Ebolavirus infection J Autoimmun 2014 Sep 23. Doi: 10.1016/j.jaut/2014.09.001. [Epub ahead of print] Level 3 • Kortepeter MG, Salwer JV, Hensley LE, et al. Real-time monitoring of cardiovascular function in rhesus macaques infected with Zaire ebolavirus. J Infect Dis 2011 Nov;204 Suppl 3:S1000-10. Animal study • Clark DV, Jahrling PB, Lawler JV. Clinical management of filovirus-infected patients. Viruses. 2012; 4, 1668-1686. Level 3 • Tan DX, Korkmaz A, Reiter RG, Manchester LC. Ebola virus disease: potential use of melatonin as treatment. J Pineal Res 2014 Sep 27. doi: 10.1111/jpi.12186. [Epub ahead of print] Level 3 • Ebola Clinical Care Guidelines: a guide for clinicians in Canada. http://www.ammi.ca/media/69846/Ebola%20Clinical%20Care%20Guidelines%202%20Sep%202014.pdf. Updated August 29, 2014. Accessed October 16, 2014. Level 3 • Feldmann H, Geisbert TW. Ebola haemorrhagic fever. The Lancet. 2011;377(9768):849-62. Level 3 • Fowler RA, Fletcher T, Fischer WA, 2nd, Lamontagne F, Jacob S, Brett-Major D, et al.Caring for critically ill patients with ebola virus disease. Perspectives from west Africa. Am J Respir Crit Care Med. 2014;190(7):733-7.Level 3 • Mupapa K, Massamba M, Kibadi K, Kuvala K, Bwaka, et al. Treatment of ebola hemorrhagic fever with blood transfusion from convalescent patients. J Infect Dis. 1999; 179(Suppl 1):S18-23. Level 2 • Roddy P, Colebunders R, Jeffs B, et al. Filovirus hemorrhagic fever outbreak case management: a review of current and future treatment options. Infect Disease. 2011; 204: S791-S795. Level 3 • Kortepeter MG, Bausch DG, Bray M. Basic clinical and laboratory features of filoviral hemorrhagic fever. Infect Disease. 2011; 204: S810-S816. Level 3 • WHO: IMAI District Clinician Manual: Hospital Care for Adolescents and Adults- Guidelines for the Management of Common Illnesses with Limited Resources, 2011. Available at http://apps.who.int/iris/bitstream/10665/77751/1/9789241548281_Vol1_eng.pdf. Level 3 • Sprecher A. Filovirus haemorrhagic fever guidelines. Médecins Sans Frontières Belgium 2013. (in draft) Level 3 • Barr J, Fraser GL, Puntillo K, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med 2013; 41:263. Level 3 See handout for evidence classification. Source: Jonathan B. Perlin, MD, PhD and HCA Management Services, L.P. 2014