IgA Nephropathy
Epidemiology. Most common lesion causing primary glomerulonephritis in the developed worldPeak incidence in 2nd and 3rd decades of life2:1 male to female predominanceMost common in Asians and Caucasians50% of new GN in Japan40% of Japanese ESRD pts10% of new US GN pts30% of new Western Europe

IgA Nephropathy
E N D
Presentation Transcript
1. IgA Nephropathy UNC Medicine Morning Report
Sally Ravanos, MD
December 5, 2008
2. Epidemiology Most common lesion causing primary glomerulonephritis in the developed world
Peak incidence in 2nd and 3rd decades of life
2:1 male to female predominance
Most common in Asians and Caucasians
50% of new GN in Japan
40% of Japanese ESRD pts
10% of new US GN pts
30% of new Western European GN pts
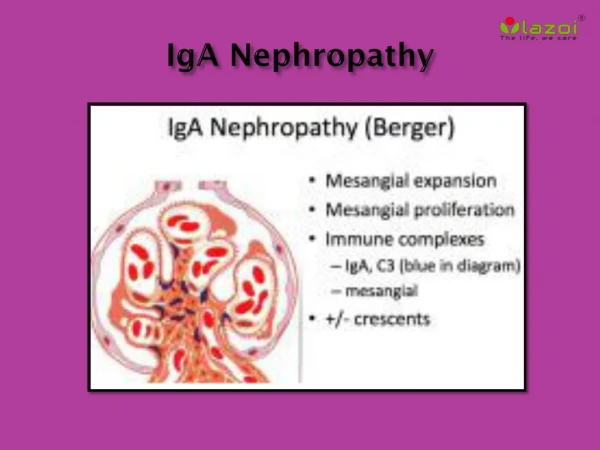
3. Pathogenesis Mesangial deposition of polymeric IgA of IgA1 subclass
IgG and complement deposition are also common
Four elements contributing to severity/course:
Synthesis/release of IgA immune complexes with characteristics that favor mesangial deposition
Ability of reticuloendothelial system to remove pathogenic IgA immune complexes or aggregates
Mesangial cell affinity for IgA accumulation
Inherent tendency of kidney to respond to injury with glomerulosclerosis and interstitial fibrosis
4. Pathogenesis (cont�d) Increased plasma IgA alone isn�t sufficient to cause disease
Anionic IgA, overrepresentation of lambda light chains
Abnormal sialylation and galactosylation in hinge regions of IgA
5. Clinical Features Three different presentations
One or recurrent episodes of gross hematuria usually following a URI (synpharyngitic hematuria)
40-50%
Microscopic hematuria and mild proteinuria incidentally detected on routine examination
30-40%
Nephrotic syndrome or acute rapidly progressive glomerulonephritis (edema, hypertension, renal insufficiency)
<10%
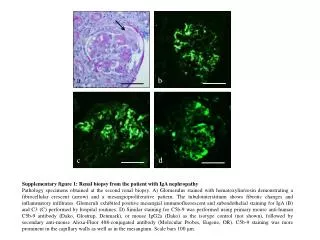
6. Diagnosis Generally based on clinical history and laboratory data
Diagnosis can only be confirmed with renal biopsy
Biopsy only pursued if signs of more progressive disease are present such as protein excretion >0.5-1g/day, elevated plasma Cr, and hypertension
7. Pathology Light Microscopy