Download
1 / 31
320 likes | 485 Views
Translation of a Transitional Care Model for Individuals with Serious Mental Illness. Nancy Hanrahan, PhD, RN, FAAN Associate Professor, School of Nursing University of Pennsylvania . Investigators & Funding.

E N D
Translation of a Transitional Care Model for Individuals with Serious Mental Illness Nancy Hanrahan, PhD, RN, FAAN Associate Professor, School of Nursing University of Pennsylvania
Investigators & Funding Funded by Robert Wood Johnson Foundation Interdisciplinary Nursing Quality Research Initiative (INQRI). No conflict of interest. Co-PI – Nancy Hanrahan, Ph.D, Associate Professor, School of Nursing, University of Pennsylvania Co-PI – Phyllis Solomon, Ph.D., Professor, School of Social Policy & Practice, University of Pennsylvania Co- Investigator, Matt Hurford, M.D. at time Assistant Professor, Dept of Psychiatry, University of Pennsylvania
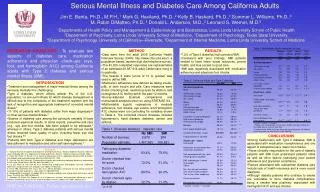
Background • SMI vulnerable after discharge from hospitalization • Especially for those with medical co-morbidities • High rates of rehospitalization, use of emergency room, homelessness, & lack of mental health treatment connection • Poor Health of Population: • Die 25 years sooner than general population (Colton & Manderschied, 2006) from treatable & preventable illnesses • High incidence of untreated hypertension, elevated blood sugar, high cholesterol, & asthma • Poor routine preventive services • Poor quality medical care • Medical comorbidities – highest need & highest cost • Top 5% of Medicaid spending • Annual per person costs $43,130 - $80,374
Background • Transitional Care Model (TCM)- an EBP for medically ill elderly • uses an advance practice nurse • Designed for elderly medical patients • 20 years of study show significant improvements in outcomes & reduced costs for high risk clients, particularly those with chronic illnesses
Background • TCM limited examination for patients with SMI • Although evidence of costly cycling in & out of hospital during exacerbation of illness of those with SMI • High cost of hospitalization in period of shrinking health care resources • Likely preventable rehospitalizations • Discharge from hospital opportune time to intervene for patients with co-morbid medical problems
Known Challenges • Patient Factors • MH problems lead to poor navigation of the health system – amotivation, cognitive deficits, & poor health literacy • System Factors • MH facilities do not provide medical care due to financing challenges & lack of expertise • Fragmentation of systems – health, mental health, & substance abuse silos of care • Complexity of MH & Health systems – different financing & policies – don’t communicate with each other
Purpose of Study • Purpose of study – to answer following questions: • Does TCM compared to usual care improve hospital to home outcomes (eg. Reduced rehosp. & ED use, & increase connection to community mental health) for discharged patients with SMI? • Is it feasible to implement & modify TCM for discharged patients with SMI? • What are the barriers & facilitators to implementing & sustaining this model? • 18 month study
Transitional Care Model (TCM) • Transitional care – broad range of time-limited services designed to ensure health care continuity, avoid preventable poor outcomes among at-risk populations, & promote safe & timely transfer of patients from one setting to another (Naylor, Aiken, Kurtzman, et al, 2011) • Emphasis on educating patients & family caregivers to address root causes of poor outcomes & avoid preventable rehospitalizations.
Background & Significance: TCM • Essential Elements of TCM • APN primary coordinator of care – assure consistency of care across episode • In-hospital assessment & develop EBP plan of care • APN home visits with ongoing telephone support (7 days per wk) for 90 days • Continuity of medical care between hosp. & primary care physician facilitated by APN accompanying patient to follow-up visits with physician
Previous Research • More recently in Canada & Scotland conducted Transitional Discharge Model (TDM) for psychiatric patients being released from hospital • Included peer support • Extension of inpatient (nurse)-practitioner (public health nurse in community) relationship prior to discharge • Nurse/ inpatient staff portion – 0-12months until community providers establish relationship with patient • Peer support aspect continues for as long as a year • 2 RCTs – one small & one large sample
Previous Research • Small sample in Scotland – reduced readmission & symptoms, & improved functioning (Reynolds, et al, 2004) • Larger sample in Canada – no difference on readmission, emergency room use, quality of life (except social relations – focus of intervention) - Length of hospital stay for experimental participants was shorter (Forchuk, 2005) • Both studies interventions were less transitional – longer term in some aspects – inpatient transition & peer support
Previous Research • Other transitional care models less medically oriented but more social service oriented post discharge from hospital, specifically, Critical Time Intervention (CTI) • CTI – 9 month intervention to support persons with SMI from institution to community living • Prevent adverse outcome by strengthening ties to services, family, & friends by providing practical & emotional support by CTI worker • Recent RCT study of formerly homeless persons discharged from 2 state hospitals to community – CTI versus usual care • Rehosp. significantly less for CTI than usual care (Tomita & Herman, 2012)
Other Models of Care • ACT – self contained team approach • Team – psychiatrist, nurse, case managers, & other specialists • May start while patient still in the hospital • Japan – J-ACT – did this • Ongoing services, high intensity – not transitional service
Methods Pilot RCT—40 participants Control Group (n=20) treatment as usual (case management provided by CMHAs) Experimental group (n=20) Psychiatric Nurse Practitioner intervention, met with patient prior to discharge, met immediately after discharge, home visits, ongoing phone calls, accompany to medical & mental health appointments, contact medical & mental health providers, medication management, 3 months duration
Advisory Group Key stakeholders: Consumers, public administrators, nurses, doctors (inpatient care), primary care doctor, home health nurses, and insurance representatives. Tasked to review and help modify TCM for the SMI Tasked to identify barriers and facilitators to implementation of TCM Met monthly throughout the study
Methods • Eligibility criteria: • 18-65 • SMI – schiz, bipolar, & major affective disorders • Major medical problem, diabetes, cardiovascular problems, cancer, etc. • Recruitment: 2 inpatient psychiatric units within a general hospital in Philadelphia • RA sat in on daily team meetings (psychiatrist, residents, nurses & discharge social worker) to screen for eligible patients for study
Methods • Outcomes • Health-related Quality of Life • Medical & psychiatric readmissions • Emergency room use • Continuity of Care • Analysis • Content analysis of Advisory Group meetings and case studies. • Statistical tests of between group differences
Sociodemographics • Sample: • Mean age 44.1 • 55% male • 45% African American • 60-75% single • 40-55% less than a high school education • 20-30% unstable housing • Mean income of $717 per month • 75% unemployed
Mental and Medical Dx Profile • Mean # of Medications: 6.1 (3.03) • Mental Disorders: • 55% Schizophrenia Spectrum • 45% Mood Disorders • Medical:
Outcome: HRQoL5 point increase=clinical sig. Physical Function, role limitation (physical), body pain, role limitation(emotional), mental Health showed a 5 point increase in both groups. Intervention showed a 10 point increase in general health compared with a 4 point increase for the control group. No other between group differences
Successful Case Example Hx – Female hosp. for manic episode; Bipolar, hypertension, non-insulin dep. Diabetes, rectal cancer, seizure disorder Barriers – overwhelmed with medical problems, appts, primary support fiancé with active substance abuse problem Facilitators – motivated to get well, providers appreciated APN APN Intervention – ed. on med. Dx & medications, coor. prescription refills, recommendations of medication with primary care physician, accompanied to medical & psychiatric appts, coor. Hosp. admission for chemo with other appts Outcome – successfully completed medical tx for rectal cancer, reconnected with Primary care physician & outpatient psychiatry and no psychiatric rehosp.
Unsuccessful Case Example Hx – 49 yrs Caucasian male; admitted for being physically aggressive & pushing boarding home staff member; Schiz paranoid; traumatic brain injury & seizure disorder Barriers – cognitive impairment & thought disorder – difficulty communicating; Boarding home unlicensed & eventually shut down Facilitators – initial contact with ICM good – but overtime less responsive; reconnected to outpt psychiatry, primary care physician & neurologist APN Int. – difficulty with anxiety & sleeping at Boarding home – APN prescribed medication; educated staff on behavioral management; initial contact with ICM Outcome – readmitted to hosp. after going to new residence & reporting suicidal ideation to psychiatrist- very aggressive while in hosp.; discharged from hosp. but returned same day - remained hosp. until end of intervention
Key Findings TCM may reduce emergency room use Continuity of Care may improve with TCM HRQoL- general health may improve with TCM Recommendation: Need further study of TCM
Key Finding • Advanced practice psychiatric nurse practitioner • Translator and ambassador role • More valued in the medical sector than mental health sector • Prescribing authority-frequent need to fill lost Rx and treat urgent symptoms. • Much time spent tracking patients and assisting with housing/social needs. • Social needs complicate medical and mental/substance use issues. Recommendations: • Integrate model into system • Team approach with a advanced practice psychiatric nurse practitioner, a social worker, a peer specialist, and a consulting psychiatrist
Key Finding • Engagement is key • Difficult to engage and conflict-ridden relationships. • Recommendation: • Greater integration of TCM early in the admission • Recovery approach • Ensure housing placement
Key Finding • Eligibility for TCM • Those with an active medical problems seemed the most responsive to the nurse intervention, therefore likely to have benefited the most. • Recommendation: • Recruit from medical side. • Focus recruitment on patients with functional problems related to medical issues
Key Finding • Poor Communication and coordination among siloed systemsa major barrier • Restrictive confidentiality policies combat stigma but prevent coordinated care • Recommendation: • Electronic MR needs to be patient-centered. • Implied consent approach e.g., circle of care
Future Directions Larger study Target medical side to recruit for the intervention Team approach Integrate TCM into hospital process to ensure more time meeting with patient prior to hospital release