Understanding the Efficacy and Challenges of Antidepressants in Treating Depression
This presentation explores the complexities of antidepressant use in the treatment of depression, drawn from extensive experience in family medicine and research. Key topics discussed include the history and context of antidepressant therapies, screening and diagnosis challenges, their effectiveness especially in pediatric and adolescent patients, and safety concerns during pregnancy. We critically evaluate the evidence supporting these medications, including common biases in research, and discuss the limitations and misconceptions surrounding their effectiveness. Gather insights into the realities of antidepressant treatment and explore alternative approaches.

Understanding the Efficacy and Challenges of Antidepressants in Treating Depression
E N D
Presentation Transcript
Depression G. Michael Allan Assoc. Prof, Family Med, U of A
Conflict of Interest Family Doctor for 12+ yrs Academic 8 years Pay from U of A and Alberta Health Research and Speaking Fees Non-Profit Sources (E.g Canadian Expert Drug Advisory Committee, Alberta College of Family Physicians, etc) No funding from Industry
Objectives • History and Context • Screening and Diagnosis • Challenges with Anti-Depressant Evidence • Do Antidepressants work? • What about pediatric (& adolescent) patients? • Safety in Pregnancy • How long do they take work? • Which is the best • Are older worse than newer? • Is one 2nd Generation better than another? • Specific Topics • What is the evidence for dose or dose adjustment? • What if the first doesn’t work? • When can we stop them?
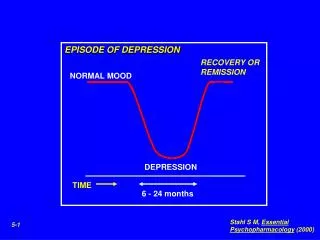
Sad Truth of Anti-depressants • Your student just saw Mrs Misery (41 y.o.). She is feeling down for 4 months, doesn’t enjoy anything, cries without cause, can’t get or stay asleep, has no energy, and can’t stay focused. She has lost 10 lbs (she is glad for that at least). • She has no thoughts of self-harm • As you write a script for an anti-depressant, the students asks, “But I thought they didn’t work?”
Sad Truth of Anti-depressants • Do Anti-depressants Work? • They work but • Not as well as we thought • It varies in some groups • Psychiatry provides the best examples of bias in the literature. • Let’s review some of those bias
Poor Quality in Anti-depressants • In a series of 46 RCT1 • 91% fair quality – 9% good (poor quality excluded) • 85% industry funded (11% affiliated, 4% not reported) • In a series of 50 RCT2 • Intention to treat used only 54% • In a series of 11 RCT3 • Allocation Concealed (assured randomization) in 9% 1) Ann Intern Med. 2005;143 :415-26. 2) Arch Gen Psychiatry 2006; 63: 1217-23. 3) Lancet 2004;363:1341-5
Other Specific Biases • Subjective: • Clinicians report/score benefit > pts • E.g.: In one series clinicians found benefit in 33% of scales but patients report benefit in 0% • Scales: • ↑ numbers (esp big scales) • Easier to find statistical significant • But not clinical significant • E.g. Improving 2.7 on a 113 scale. Lancet 2004;363:1341-5. & BMJ 2004;328:879-83.
Hiding the Bad: Part 1 • Selective Publication of Anti-depressant Trials • FDA records of 12 SSRI/SNRI’s vs Published • 74 Trials: • 38 Positive: 37 published, 1 not published. • 36 Negative: 3 published as negative, 11 published as positive, 22 not published. • Positive = 94% published vs 51% FDA • Effect (benefit): Published (0.41) > FDA (0.31) NEJM 2008; 358: 252.
Hiding the Bad:Part 2 • Single Trails Pub: • if trial +ve = 90% • if trial –ve = 29% • What Actually happens to SSRI trials? • Hiding “Bad” trials • Multiple pub. “Good” Melander. et al, BMJ, 2003; 326: 1171-73
Hiding the Bad: Part 2 • What Actually happens to SSRI trials? • +ve trials published 4.4x each (vs 1.3) Melander. et al, BMJ, 2003; 326: 1171-73
Getting the most of a small effect • Initial Severity and Anti-depressant Benefits • 35 RCT’s of 4 SSRI/SNRI’s • No diff. between Anti-depressants • Overall, Statistical Sign common BUT,… • Clinical Significance less clear • Ham D scores range between 17-30.5 • Mean Change was 9.6 for med & 7.8 for placebo • Mean difference was 1.8 HRSD • Therefore, 81.5% of the improve seen on anti-depressants is from “placebo” PLOS Med 2008; 5(2): 0260.
These are basically scatter plots with regression analysis. • Putting on mean outcomes for placebo and drug from each trial and drawing a best fit line for the effect of placebo and drug. • You then figure out when the two separate to predefined level. • This uses effect sizes, which is common in summary statistics for scales (like depression or pain) • In this case, they used 0.5 which they got from NICE. • It separates at green, about HSRD 27 • Note: If they used an easier clinical sign (let’s say 0.2, like in OA), separation would be earlier (around 24 in the OA case). Effect size
Getting the most of a small effect • Differences Only reach Clinical Significance when Depression Severe • The actual number varies by graph but seems like HSRD 26 (from figure 4), 27 (from figure 3) and 28 (from figure 2) • Maybe lower (perhaps Moderate) if “clinical significance” defined more liberally • Example: 0.2 is defined as the minimum effect size in OA • Bottom-line: drug effect stable but placebo less effective as depression worsens • Meaning, benefit of drug over placebo greater with worsening depression. PLOS Med 2008; 5(2): 0260.
Getting the most: NEW • Meta-analysis of 6 trials: with patient level data! • Searched 3 databases (pubmed, Psychinfo & cochrane). • RCT, Adult, ≥ 6 wks, Ham D, pt level data. • 6 studies (3 imipramine, 3 Paroxetine), 6-11 weeks (median 8), baseline Ham D= 14-23. • Results: Same as before, severe, benefit • Clin Sign Diff (NICE definition (diff 3 on Ham-D) at Ham-D 25
Getting the most: NEW • Continued results: used 3 categories • Mild/mod (Ham-D ≤18), severe (19-22), very severe (≥23) • Using effect size (measuring diff from comparator): both mild/mod & severe never got better 0.20. At very severe 0.47. • NNT (for better outcome): 16, 11 and 4 (mild/mod, severe, very severe). JAMA. 2010;303(1):47-53
Getting to the Actual Numbers • Paroxetine is well studied and a meta-analysis of the drug helps see the individual outcomes • Standard Mean difference was -0.31, -0.40 to -0.22) • Actual numbers that get ≥50% of improvement; If you treat 100 pts with paroxetine • 53% taking paroxetine • 42% with placebo • Difference is 11% (or NNT 9) • If you look at other outcomes • Those who discontinue for any reason: no difference • Adverse events: reporting (NNH 9), discontinuing due to (NNH 17) • Experience Suicidal tendencies (NNH 142).* CMAJ 2008;178(3):296-305
Bottom-line • Antidepressants help reduce symptoms of (moderate to severe) depression in up to 70% of patients • (but likely lower & maybe a lot lower) • Remission Less. • In mild Depression, 90% of that effect is from “Placebo” • As the Depression is more severe, the drug gives more of that effect (compared to placebo).
Best Anti-depressant • A 27 year old woman has been slipping into depression for 4 months and non-medicinal measures have been ineffective. She is now clearly depressed (not suicidal). You have heard from psychiatrists and different drug reps certain meds are better.
Best Anti-depressant • Which was better in a well-designed meta-analysis? • Venlafaxine • Buproprion • Esocitalopram • Citalopram • They’re all the same • None Ever Work (Dr Thomas Cruise)
Best Anti-Depressant = Any • They are all about the same • 46 RCT’s (11.5 K pts), ≥3 months • No Diff Quality of Life (& for Ham D) • Venlafaxine > Fluoxentine: RB 1.12 (1.02-1.23) & NNT16 • Sertraline > Fluoxetine: RB 1.1 (1.01-1.2) & NNT 17 • SE similar (? Venlafaxine N&V), rapidity of response No diff. • Benefit = always 5% in favour of sponsored drug (NNT 20) • SE similar (? Venlafaxine N&V), rapidity of response No diff. Ann Intern Med. 2005;143 :415-26.
Best Anti-Depressant = Any • Added since 2005 • Meta-analysis1: 203 studies (171 RCT’s) – using some indirect comparisons • Effectiveness similar. Few stat sign relative benefit, but • None clinically significant E.g. MADRS 60 pt scale: esocitalopram 1.13 > citalopram (min clinically important diff=2) • Sponsorship may play a role in these subtle differences • Adverse Events similar in amount (61% of patients had ≥1) but types varied • E.g. Venlafaxine 11% more nausea & vomiting, Sertraline 3% more diarrhea, 1. Ann Intern Med. 2008;149:734-750. 2. Lancet 2009; 373: 746–58
Best Anti-Depressant = Any • Meta-analysis2 (117 RCTs), examined response to treatment and withdrawal, used indirect methods • Identified some small differences • Efficacy Top 4: mirtazapine, escitalopram, venlafaxine, sertraline • Acceptability Top 4: escitalopram, sertraline, bupropion, citalopram • Used Odds Ratios, treated scales as =, Funding bias • Interpret in context 1) Antidepressant research suffers significant bias, 2) ≤10% of studies are high quality • Bottom-line: Similar Effectiveness, different AE 1. Ann Intern Med. 2008;149:734-750. 2. Lancet 2009; 373: 746–58
Best Antidepressant = Any: Quality Concerns • Other reviews have attempted to determine if one antidepressant is superior but the results are inconsistent.1 • The 2009 review2 has important concerns regarding validity including, • They treated all depression scales as the same (and they are not), • Using odds ratios exaggerated the differences they found, • Importantly, when they tried to account for sponsorship bias, the differences between the drugs were reduced. • Both reviews2,3 did some indirect comparison of drugs from different studies, which is less reliable than direct comparison in the same study. • The 2008 review3 did not have quite as many concerns with validity. 1) Cochrane 2005;(4): CD004185. Curr Med Res Opin. 2009; 25 :161-75. Cochrane 2009;(2): CD006117. Ann Intern Med. 2005;143 :415-26. 2) Lancet 2009; 373: 746–58. 3) Ann Intern Med. 2008;149: 734-750.
Is Bigger Better? • Mrs Low (31 year old) is in. 2 weeks ago she was diagnosed with moderate depression. She is now ready to trial a medication. • Your resident says he heard (from an expert) that “primary care doctors always under-treat depression” • As you write the script, he wants to know what your target dose is.
Is Bigger Better • Based on two literatures reviews, you can say; • Moderate dose SSRI (e.g. 30-40) is the general target • Starting low (10mg) is reasonable • Increases into high doses (>20mg) may not be much help. • Forget the prescription, send her to this know it all expert.
Bigger Is NOT Better • Low doses of anti-depressants seem as effective as high doses. • Flouxetine (5 vs 20 vs 40mg)1 • Tricyclics (50-100 vs >100mg)2 • Increasing doses in non- responsive patients doesn’t seem to help much.3 • At least not until 8 weeks have past. 1) Psychopharm Bull 1988; 24: 183-8. 2) BMJ. 2002;325:991-5. 3) Br J Psychiatry 2006;189:309–16.
Switching Quick: New What constitutes a reasonable trial? When should we say, “this isn’t working, lets’ try another instead.” Only three studies have looked at this and can’t see a difference in switching after 6-7 weeks and not. Note STAR*D waited a mean of 12 weeks Acta Psychiatr Scand 2010;121:174–9.
New: Combination • Combined regular anti-depressants at the start may be helpful, • RCT of 105 pts x 6 weeks, Fluoxetine (20) vs Mirtazapine (30) plus Fuoxetine (20) or Venlafaxine (225) or Bupropion (150) • Remission = Ham D ≤7 (mean start =22) • Fluox 25%, Fluox+M 52%, Ven+M 58%, Bup+M 46% (all comb stat sign (p=0.01) vs Fluox alone); NNT 4 • AE common but No diff in AE quiting • Few other studies also find (nothing big yet though). Am J Psychiatry 2010; 167:281–288
Waiting for the World to Change • Mrs low is back 7 days later. She is on Fluoxetine 10mg. She reports she is feeling a little better (more energy concentration). • She read that it should take 2-4 weeks to work so wants to know how this can be helping? • How fast do anti-depressants work?
Waiting for the World to Change • They work as fast as 7 days: • From a meta-analysis1 of 50 trials (10,121 depressed patients) looking at response to SSRI medications, compared to placebo, at a series of time intervals. • On average, 1/3 of the total benefit occurs in the first 7 days (whole effect by 6 weeks). • For every 25 people treated, one more will be 50% improved over placebo at 7 days. • Hard to find because the “n” needed to show a benefit is 9x bigger that most trials! • The results of the meta-analysis above confirm those of another meta-analysis2 • That study also found antidepressants result in statistically significant improvement in clinically important outcomes within the first week. 1) Arch Gen Psychiatry 2006; 63: 1217-23. 2) J Clin Psychopharmacol 2006;26:56–60.
A Trial of Separation? • Mrs Low is now 6 months on Anti-depressants and has done well. This was her first case of depression. She wants to know if she can stop? • What if this was her 2nd or 3rd case?
A Trial of Separation? • In Meta-analysis of 31 RCT (of all types)1 • Meds stopped after 4-28 weeks (most 6-16) • Relapse at 12 months: 41% Placebo vs 18% • NNT 5. • Dose reduction similar (5 RCT)2 • 25.3% low dose vs 15.1% in previous dose • Recurrence (hard to separate out one)3 • From a cohort of 318 depressed pts, 60% had previous depression • After 1 yr, 25% of the cohort had a recurrence • If second, 41% in 1 year. • Add 16% for each subsequent episode, but some repeaters • 36% did not have a recurrence in 5 years. 1) Lancet 2003; 361: 653–51. 2) Psychother Psychosom. 2007;76(5):266-70 3) Am J Psychiatry 2000; 157:229–233
Missing the Diagnosis • Ms V Blue is a 25 year old female coming for her complete medical. She is mentions she is a little more fatigued of late. • You want to screen for depression. • Is there a quick screen?
2 Question Screen • During the past month have you often been bothered by, • Feeling down, depressed, or hopeless? • Little interest or pleasure in doing things? • No to both: virtually rules out depression • LR 0.05 (Sensitivity 97%) • Yes to either: go through full depression questions • Not specific (can’t make Dx, many false positives) • Another study of these found same (LR 0.07) BMJ 2003; 327:1144-46.J Gen Intern Med. 1997;12:439-45.
Patients Like Ours? Shooting Stars: Fall to Earth • So what really happens to the average patient seen for depression?
Shooting STAR*D: Findings • 2876 people were put on Citalopram • More like real patients • (mix of general and specialty) • 80% had chronic or recurrent depression • Many complicating Psychiatric conditions. • 18% had attempted suicide. • Mean HRSD = 21.8 • Mean exit dose of citalopram = 42 mg/day
Shooting STAR*D: Findings • Citalopram remission rates • HRSD = 27.5% and QIDS-SRTreatment 33% • Response rate = 47% • Similar rates between GP’s and specialists • If a patient hadn’t attained remission, they were offered to continue. • 2086 patients were offered to continue. Am J Psychiatry 2006; 163:28–40
Shooting STAR*D: 2 Findings • Substituting 727 patients • Drop Citalopram and immediate start: • Bupropion-SR, Sertraline, or Venlafaxine-XR • Remission rates about 25% across the board (for both tools & all 3 meds). • Tolerability and adverse events similar. N Engl J Med 2006;354:1231-42.
Shooting STAR*D: 2 Findings • Augmenting 565 patients • Drop Citalopram continue and add: • Bupropion or Buspirone • HSRD Remission rates around 30% for both. • QIDS-SR-16: Buproprion > than buspirone • Reduction 25% vs 17% • Lower end score 8 vs 9 • Lower intolerance drop-out rate 12.5% vs 20.6 N Engl J Med 2006;354:1243-52.
Shooting STAR*D: 3 Findings • Augmenting 142 patients • Add: Lithium or triiodothyronine (T3) • Remission rates around 20% for both. • Substituting 234 patients • Switch: nortriptyline or mirtazapine • Remission rates between 10-20% for both EBMH November 2008; 11(4): 97-9.
Shooting STAR*D: Summary • Perhaps trials reporting the ideal response 70% (or more “realistic” 53% from the paroxetine study) are actually an exaggeration • Efficacy population = 51.6% response versus 39.1% in effectiveness or pragmatic STAR*D population. • Maybe choosing the type of alternative antidep doesn’t matter (they seem the same). • Maybe specialist care is not a lot different from GP • Choice of augmentation uncertain (guidelines2 put lithium and olanzapine ahead of the first choices here). Am J Psychiatry 2009; 166:599–607. 2. J Psychopharmacol 2008;22:343–96.
Related to STAR*D: New • Cochrane Database Syst Rev. 2009 Jul 8;(3):CD007954. • J Clin Psychiatry. 2006 Dec;67(12):1836-55. • Some related citations • Treating Depression in Primary Care does work1 • Treatment response NNT 7-9, • Withdrawal due to AE (4-30 TCA or 20-90 SSRI) • If you need to switch,2 • it doesn’t matter which one • The more previous treatments, the higher the chance of a poor outcomes.
Pediatric Depression: Meds or not You are seeing a 12 year old boy whom a has many symptoms of depression. This is new for him (last 6 weeks). His mother worried and wonders if antidepressants might help (she has been successfully treated in the past). In addition to possible referral, looking into contributing factors, etc: What can we say about antidepressants in pediatrics.
Pediatric Depression: Meds or not • What can we say: • There are concerns that the drugs are ineffective. • There are concerns that the drugs are not safe. • There is some evidence that perhaps fluoxetine may be a reasonable choice. • SR/Met: 5 Databases + refs & authors, 6 drugs (5 pub, 6 unpub from 5000+), f/u 42-96 days F/U poor (54-83%). (BMJ= 4 drugs, 6 published trials) Lancet 2004;363:1341-5 (BMJ 2004;328:879-83)
Pediatric Depression: Meds or not New anti-depressants vs placebo Results: see table Good use of unpublished data, excellent combo, but poor f/u, short duration Industry bias (under-reporting SE & Hiding trials). Fluoxetine only (for now) & Some question it’s benefit. Lancet 2004;363:1341-5 (BMJ 2004;328:879-83)
Study 1 & 2: SSRIs in childhood dep,… & Efficacy & safety of anti-depressants,... In 6 trials, 42 measures used but only 14 showed any improve (0/10 patient/parent measures. Scales clinically questionable (Improving 2.7 on a 113 scale ?)
Suicide • Adolescents: Odds ratio 1.92 (1.51-2.44) • Adults: 0.57 (0.47-0.70) • Elderly: 0.46 (0.27-0.79) • Absolute numbers not given (but likely low). CMAJ. 2009;180:291-7.