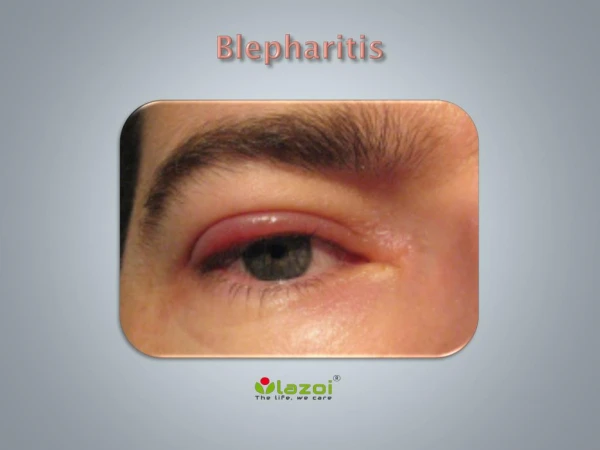
Posterior Blepharitis
Posterior Blepharitis. Referred to as Meibomian Gland Dysfunction (MGD): The normal secretion of the MG becomes thick and yellow-white instead of free-flowing & clear. Primary MGD affects all the meibomian glands associated with staphylococcal blepharitis.

Posterior Blepharitis
E N D
Presentation Transcript
Posterior Blepharitis • Referred to as Meibomian Gland Dysfunction (MGD): • The normal secretion of the MG becomes thick and yellow-white instead of free-flowing & clear. • Primary MGD affects all the meibomian glands associated with staphylococcal blepharitis. • Secondary MGD occurs in a spotty fashion associated with seborrheic blepharitis.
Pathogenesis of MGD: • Meibum which is different than sebum (produced in the skin). Normal meibum has a melting point equal to or lower than the ocular surface temperature. • Obstruction of the meibomian ducts from any source leads to bacterial colonization and the altering of the normal meibum. • Abnormal meibum doesn’t allow for normal corneal wettability. • Abnormal meibum has a melting point above the ocular surface temperature, which causes it to solidify and obstruct the ducts.
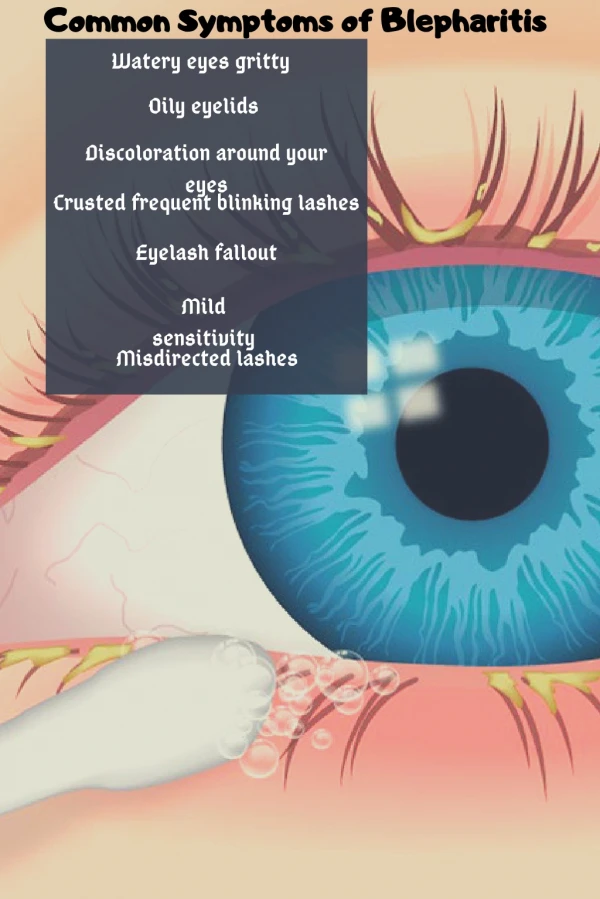
Clinical Appearance of MGD: • MGD’s are not always seen with inflammatory signs & often missed. • Signs: • Inspissated plugs at the opening of the meibomian glands. • Yellow-white secretions on expression • Foamy discharge into the tear film • Thickened, rounded lid margins.
Meibomian Gland Dysfunction: • Note: • Blocked Meibomian Glands, Meibomian plugs (Inspissated plugs). • Associated Anterior Blepharitis. • Fine blood vessels (telangiectasia)
Meibomian Gland Dysfunction: Expression of Meibomian glands
Meibomian Gland Dysfunction: Corneal complications: 1) Dry eye 2) Punctate Keratitis
Management of MGD: • Hot compresses followed by digital massage 2 – 4 times daily. • For moderate to severe cases you can consider oral tetracycline (250mg QID). * Who cannot receive this med? 3) Treat the dry eye which is almost always present.
External Hordeolum: • AKA “stye”. • An acute Staph infection of the glands of Zeis and Moll. • Associated with Blepharitis. • Often associated with fatigue, poor diet and stress. • Can be recurrent.
External Hordeolum Signs: • Localized redness and pain of recent onset. • The lesion will begin to “point” within a few days.
External Hordeolum “Pointing” • This will often spontaneously drain in 3 – 4 days.
Management of External Hordeolum: • Hot compresses several times daily will hasten pointing and drainage. • Topicals? • Epilate an associated lash. • Stab incision without anesthesia. • Oral antibiotics (erythromycin, dicloxacillin, tetracycline)
Dicloxacillin: Q: What type of antibiotic? A: Penicillin Q: How does it work? A: Inhibits Cell Wall synthesis Q: Most common side effect? A: Hypersensitivity Dosage for skin infections? 125 – 250 mg QID x 10 to 14 days.
Internal Hordeolum: • A localized infection of the meibomian gland with obstruction. • Onset and course is longer than external hordeolum • Treat with warm compresses or oral antibiotics (No topicals).
Angular Blepharitis: • Bacterial infection of the medial or lateral canthal area. • Hyperemia, desquamation (crusting) and discomfort in the involved area. • Conjunctiva can be involved. • Treat with 0.25% zinc sulfate solution applied with cotton-tip applicator 3-5 times daily. Topical antibiotic ung works as well.
Any Guesses now? Phthirus pubis
Phthiriasis palpebrarum • An uncommon eyelid infestation of Phthirus pubis (crab louse). • Occurs when sanitary conditions are poor. • Can be transmitted from bedding and towels. • Treatment consists of thick ung applied to lids to smother the parasites. • Epilate lashes.
Canaliculitis: • Symptoms: - Red eye resistent to antibiotic therapy. - Tearing (Epiphora) • Causes: -Actinomyces (but can be herpetic or allergic)
Actinomyces: Q: A Bacteria? A: Yes Generally responds to topical and oral therapy if the concretions are removed. DacryoCystoRhinostomy DCR Patients over 50.
Antibacterial Treatment for Canaliculitis: Topical • Combination of neomycin, bacitracin, polymyxin B (Neosporin) • Applied q3 – 4h x 7 to 10d. Oral • Penicillin or Ampicillin (250 – 500 mg QID)
Dacryocystitis: • In children S. aureus and H. influenzae. • In adults S. aureus, S. epidermidis, and Pseudomonas. * Anaerobes can be present. • Culture and sensitivities recommended.
Dacryocystitis: • Swelling limited upwardly by the medial canthal ligament. • Pain and redness differentiates this from a mucocele which is nontender. • Managed with cloxacillin or dicloxacillin
Dacryocystitis vs. Mucocele • Mucocele – A cystic mass usually filled with mucous. Typically arises after sinusitis.
Preseptal vs. OrbitalCellulitis: Preseptal Cellulitis: An infectious process involving the lid stuctures anterior to the orbital septum. Occurs: 1) Secondary to localized infection of the lids. 2) Secondary to lid or facial trauma. 3) After an Upper Respiratory Tract Infection. **Most common cause is Group A Streptococci.
Preseptal vs. OrbitalCellulitis: Both Conditions show: • Chemosis • Conjunctival injection • Pain • Redness • Swelling of the lids
Preseptal: No Proptosis F.R.O.M. of EOM’s Normal Pupils Normal Visual Acuity Orbital: Proptosis Ophthalmoplegia + APD Reduced Visual Acuity Preseptal vs. Orbital Cellulitis:
Preseptal vs. Orbital Cellulitis: If examination of the pupils, EOM and VA is not possible. Consider a CT.
Laboratory Testing in Cases of Preseptal & Orbital Cellulitis • Complete Blood Count with differential • Temperature – elevated in Orbital. • Blood Cultures – helps to establish a cause in children. Rarely positive in adults. Pus from draining wounds can be cultured • 12% to 25% of patients with Haemophilus preseptal or orbital cellulitis have concomitant meningitis.
Management of Preseptal Cellulitis Oral Antibiotics: • Mild to moderate presentations respond to dicloxacillin or cephalexin. • Medication should continue for 10 days. • IV antibiotics should be considered in severe cases.
Cephalexin: • A first generation cephalosporin. Like the penicillins they contain the ß-lactam ring. • Trade names include Keflex, Keftab and Biocef.
Management of Orbital Cellulitis There is significant potential morbidity and even mortality as a post-septal lid infection can spread through a valveless venous system leading to cavernous sinus thrombosis, meningitis, intracranial infection, and septicemia. ** Immediate hospitalization ** IV Antibiotics
Is this a cellulitis or something different? Dacryoadenitis: • Characterized by swelling in the temporal one-third to one-half of the upper lid (S-shaped). • Can be bacterial (Mycobacterium or Neisseria). • Managed with IM antibiotics.