Download
1 / 119
1.7k likes | 2.66k Views
NUCLEAR MEDICINE THE BASICS. LTC Aaron L. Stack, M.D. Nuclear Medicine Service WRAMC Assistant Professor of Radiology and Nuclear Medicine, USUHS. What is Nuclear Medicine?.

E N D
NUCLEAR MEDICINE THE BASICS LTC Aaron L. Stack, M.D. Nuclear Medicine Service WRAMC Assistant Professor of Radiology and Nuclear Medicine, USUHS
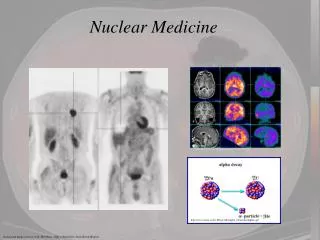
What is Nuclear Medicine? • Administration of radiopharmaceuticals, whether oral, IV, intra-paritoneal or intra-articular, for the purpose of imaging, diagnosis or treatment.
What is Nuclear Medicine? • According to Wikipedia: • Nuclear medicine is a branch of medicine and medical imaging that uses unsealed radioactive substances in diagnosis and therapy. These substances consist of radionuclides, or pharmaceuticals that have been labeled with radionuclides (radiopharmaceuticals).
Why Nuclear Medicine? Diagnosis?
Imaging Studies • Too Numerous to list • Bone Scan • Myocardial Perfusion • PET, PET/CT • V/Q Scan • HIDA Scan • Renal Lasix Study • GI Bleed Study • Thyroid Uptake and Scan • Tagged WBC Studies • Brain Perfusion/CSF Flow • Renal Cortical Scan • Nuclear Cystogram • Gastric and Esophageal Emptying • Parathyroid Imaging
Non-Imaging Studies • GFR • H-Pylori • I-131 Dosimetry • Iodine Uptake • Blood Volume
Therapeutic Procedures • I-131 Therapy (hyperthyroid) • I-131 Ablation (cancer) • Zevalin and Bexxar – Refractory Non-Hodgin Lymphoma Treatment • Strontium and Samarium Bone Pain Therapy • Polycythemia Vera Treatment
How does this stuff work? • Gamma ray emission • Radionuclide production • Getting the gamma ray to the right spot • Radiopharmaceutical injection • Imaging the gamma rays • Gamma cameras • Producing usefull information from images • Collimation, filtering, electronic discriminators, electronic amplifiers
What Are Gamma Rays? • Gamma rays are an energetic form of electromagnetic radiation produced by radioactive decay or other nuclear or subatomic processes such as electron-positron annihilation.
What Are Gamma Rays? • The difference between gamma rays and X-rays is their site of origin. • Gamma rays are photons that originate in the nucleus of the atom. • X-rays are photons that originate outside the nucleus (an outer electron shell).
What is Alpha, Beta and Gamma? • Alpha radiation is basically a Helium nucleus (2 protons and 2 neutrons with a +2 charge). • Alpha radiation is common in the higher Atomic Number range of the Periodic Table. • Radium-226 decays by Alpha Decay to Radon-222.
What is Alpha, Beta and Gamma? • Alpha Radiation loses all of its energy very quickly, so it can only travel a fraction of a mm in tissue. • A sheet of paper can stop alpha particles. • Not useful in imaging.
What is Alpha, Beta and Gamma? • Beta Radiation refers a positively (positron) or negatively (negatron) charged electron being emitted from the nucleus.
What is Alpha, Beta and Gamma? • Beta Minus Decay occurs in a neutron-rich environment. This results in conversion of a neutron into a proton, an electron and an anti-neutrino. The electron is ejected from the nucleus, thus the name negatron or Beta Minus decay.
What is Alpha, Beta and Gamma? • Beta Plus decay occurs in a neutron-poor environment. This results in a positively charged particle equivalent to an electron being ejected from the nucleus, converting a proton into a neutron.
What is Alpha, Beta and Gamma? • Beta Radiation can travel up to a few mm in tissue and can have a significant damaging effect on surrounding tissues. • I-131 is a classic Beta - emitting radionuclide. • I-131 used to treat thyroid disorders and cancer. • F-18 FDG is the most widely used Beta-Plus decay radiopharmaceutical, used in PET imaging.
What is Alpha, Beta and Gamma? • Gamma Rays are ionizing electromagnetic radiations that originate in an unstable, excited atomic nucleus. • Each radionuclide has a discrete energy or energies of decay emission, according to its decay scheme. • Energies useful in nuclear medicine range between 80 and 400 KeV.
How Does a Gamma Camera Work? • Radiotracer mimicks a physiologic process • Imaging equipment • Collimator • Crystal • Computer processing (SPECT, Gating, Cine) • Image display (monitor, film, counts)
How Does a Gamma Camera Work? • The system accumulates counts of gamma photons that are absorbed by a crystal in the camera, usually a large flat crystal of sodium iodide with thallium doping in a light-sealed housing.
How Does a Gamma Camera Work? • The crystal scintillates in response to incident gamma radiation: when a gamma photon knocks an electron loose from an iodine atom in the crystal, a faint flash of light is produced when the electron again finds a minimal energy state.
The Main Players • IsotopeDecayT-1/2EnergyProduction • Tc99m IT 6 hrs. 140 KeV Gener. • I-123 EC 13 hrs. 159 KeV Cycl. • I-131 B- 8 days 364 KeV Reactor • Tl-201 EC 73 hrs. 69-83 KeV Cycl. • In-111 EC 68 hrs. 171, 245 Kev Cyc. • Xe-133 B- 5.2 days 81 KeV Reactor • F-18 FDG B+ 110 min. 511 KeV Cycl.
The Important Studies • Emergency/Urgent Studies • How we do them • Why they work • How we interpret them • How good are we • Pitfalls • Examples
Case Studies • V/Q Scan • Bone Scan • Thyroid • PET (F18-FDG) • HIDA Scan • GI Bleed Scan
V/Q Scan • Ventillation • Xe-133 Gas inhaled through closed system • Initial breath hold, Equalibrium, Washout • Perfusion • Tc99m-MAA • Injected supine • Imaged supine or upright, multiple oblique views.
V/Q Scan • Ventillation • Xe-133 shows overall ventillatory pattern of lungs. Very accurate. • Lipophyllic – will diffuse into blood stream and if fatty liver, will accumulate in liver. • Identifies moderate to large areas of hypoventillated lung.
V/Q Scan • Perfusion • Tc99m-labeled Macro Aggregated Albumin particles. Particles range in size from 5 – 100 microns. (60-80% 10-30 um). • Typically 200,000 to 700,000 particles are administered in an adult (minimum 100K) • Decreased in Peds, ½ particles in pulmonary HTN, known shunt or pregnancy.
V/Q Scan • Ventillation done first. Activity washes out from lungs rapidly, does not interfere with perfusion study. • MAA injected with Pt. supine to allow even distribution throughout upper, mid and lower lungs. Two minutes after injection, images acquired. MAA lodges in capillaries. • Estimated 300 million pre-capillary arterioles and over 280 billion pulmonary capillaries. • Occlusion or partial occlusion of only 0.1 – 0.3 % of pulmonary vessels.
V/Q Scan • Interpretation • Must have accompanying CXR • Symptoms must be acute (<48 hrs.) • PIOPED Guidelines for estimating probability of Pulmonary Embolism • Gestalt interpretation used by experienced readers
Pulmonary Embolism • Clinical risk factors (PIOPED) • Immobilization for a min of 3 days • Surgery within 3 months • Factors that were not reliable: • Dyspnea • Pleuritic chest pain • Tachypnea • Other chest symptoms
Pulmonary Embolism • Chest radiographs • 80% of PE patients had an abnormal chest radiograph • Atelectasis • Parenchymal opacity • Commonly patients without PE also had parenchymal abnormalities • A small pleural effusion with a matched V/Q defect was a better predictor for the presence of a PE than a large effusion with a V/Q defect
PIOPED • Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) • Nuclear Medicine Working Group – 1983 • Criteria field test – 1984 • Finalized criteria, enrollment start – Jan 1, 1985 • Investigators recognized that some of the criteria to be tested would be invalid
Original PIOPED • Segmental perfusion defects size • Small – less than 25% of a segment “rat bites” • Moderate – 25-75% of a segment “subsegmental” • Large – greater than 75% of a segment “segmental” • Lobar need not apply! segmental anatomy only! • Assumption: partially occluding emboli may cause decreased but not absent perfusion
Original PIOPED • Results Satisfactory or better: • Perfusion scan 96% • Ventilation scan 95% Reader agreement 90% • High 95% • Intermediate 75% • Low 70% • Very Low 92% • Normal 94% Less than 3% required panel discussion
Revised PIOPED • Gottschalk A, Sostman HD, Alavi A, et al. Ventilation-Perfusion Scintigraphy in the PIOPED study. Part II. Evaluation of the scintigraphic criteria and intrepretations. J Nucl Med 1993;34(7):1119-1126. • Used the computerized data obtained in the original study • Evaluate the criteria for categorical interpretation of V/Q scans • Estimate the percent probability of pulmonary embolism
Revised PIOPED • These results were compared to the PIOPED Angiography Working Group data • Pulmonary emboli were identified by location, making comparison with the V/Q data possible • Patients without ventilation scans were not included • Patients which were clinically asymptomatic at 1 year without anticoagulation were not considered to have experienced a PE (no angio group)
Revised PIOPED • High Probability (> 80%) • > 2 Large (>75% of a segment) mismatched segmental perfusion defects or the arithmetic equivalent in moderate or large + moderate defects.
Revised PIOPED • Intermediate Probability (20%-79%) • One large to two moderate mismatched segmental perfusion defects or the arithmetic equivalent in moderate or large + moderate defects • Single matched ventilation-perfusion defect with clear chest radiograph. • Triple matched defect(s) in lower lung zone • Difficult to categorize as low or high, or not described as such.
Revised PIOPED • Low Probability (< 20%) • Nonsegmental perfusion defects (cardiomegaly, enlarged aorta, enlarged hila, elevated hemidiaphragm). • Any perfusion defect with a substantially larger chest radiographic abnormality. • Perfusion defects matched by ventilation abnormality provided that there are: (1) clear cxr and (2) some areas of normal lung perfusion. • Triple matched defects in upper or mid lung zones • Any number of small perfusion defects with a normal cxr.
Revised PIOPED • Very Low Probability • Ceased to exist! • Normal • No perfusion defects present. • Perfusion outlines exactly the shape of the lungs as seen on the chest radiograph (hilar and aortic impressions may be seen, chest radiograph and/or ventilation study may be abnormal).
Revised PIOPED Probability % • Normal < 4 • Low 0 – 19 • Intermediate 20-79 • High 80-100
Baseline Acute symptoms