Download
1 / 43
430 likes | 555 Views
Sheila Mac Neil Professor Of Tissue Engineering and founder Director of Celltran Ltd Ethical & legal challenges to Stem Cell research. Sheila MacNeil University of Sheffield Skin Forum Sheffield June 2006. Stem Cell Research and Tissue Engineering. Contents.

E N D
Sheila Mac NeilProfessor Of Tissue Engineering and founder Director of Celltran LtdEthical & legal challenges to Stem Cell research Sheila MacNeil University of Sheffield Skin Forum Sheffield June 2006 Stem Cell Research and Tissue Engineering
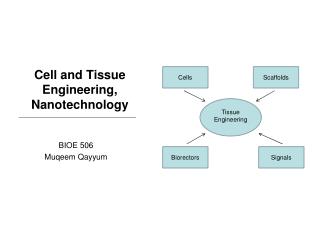
Contents • Tissue engineering research using adult cells Skin-burns patients Skin-chronic ulcers Oral mucosa-scarring of the urethra Melanocytes-vitiligo Corneal epithelial cells-corneal diseases • Ethical Regulatory and Economic issues
Do we have stem cells in our cultures? • Adult epithelial cells (skin, oral mucosa and cornea) cultured in the laboratory contains cells with colony forming ability which give rapid expansion • Patients who received cultured skin in the 1980’s still doing well-no loss of skin • Concensus view is that culture protocols maintain a population of cells with “stem like” properties but that without gene manipulation these are destined to give rise to only one tissue
A wonderful stuff is skin. It’s the stuff that keeps you in” Spike Milligan
There had to be a simpler way to get cells to patients… • Professor Rob Short-Surface Engineer • Professor Sheila MacNeil-Tissue Engineer “Lets make a post-it note for delivering skin cells to patients” 1997
Celltran Ltd • University of Sheffield spin-out company • Formed 2000 • 16 staff • MHRA approved cleanrooms in 2003 • Launched Myskin in 2004 • Merged with Xcellentis in 2006 • Raised 5 Million in funding • Full details of development and proof of concept clinical studies with myskin available on www.celltran.co.uk
Myskin™ • Autologous keratinocytes • Proprietary materials technology • Chronic wounds, burns • DFU/VLU trials • Case studies • Revenues since April 2004
Wound bed preparation – debride and optimise* myskin surface -2 days Week 0 Week 1 Weeks 2-6 Cell expansion at CellTran laboratory Thin shave biopsy taken and delivered to CellTran Myskin couriered to patient Repeat myskin delivery as required Wound healing Patient Information Cryogenic cell storage myskin process
Use of Myskin for failed skin grafts Patient 5Male, 80 years old Right leg before applications 4 weeks non-healing After 12 applications – 78% healed, suitable for grafting 2 months post treatment
What types of patients can benefit ? • Acute burns-where it provides valuable adjunct to SSG and donor skin • Chronic wounds-BUT-the earlier it is used the better the outcome and the fewer applications will be needed • Chronic wounds of long standing may need pretreatment to improve the wound bed prior to application
Development a carrier surface for surgical treatment of vitiligo Cells on carrier surface Biopsy
MTT of carrier dressing S100 Mel-5 Melanocytes MTT of fresh skin Melanocytes Transfer of melanocytes and keratinocytes from carrier to in vitro human wound bed model
Contact lens seeded with limbal epithelial cells Stroma Agar Sclera Organ culture Contact lens Developing a coated contact lens as a carrier for cultured corneal cells for corneal diseases
Tissue engineered skin and oral mucosa for reconstructive surgery • Tissue engineered skin for release of contractures due to earlier burns injuries • Tissue engineered oral mucosa for replacing chronically scarred urethral tissue
Ethical, Regulatory and Economic issues Ethical issues • Why do this? -Because existing clinical treatments not adequate for job • What is the risk versus the benefit for patients? • What can go wrong? How likely is it? • Obtaining Ethical Committee consent • Making sure patients are fully informed and properly consented
Ethical, Regulatory and Economic issues Ethical issues-in practice • Patients very willing to use own tissues (small biopsy) for burns, chronic wounds and reconstructive surgery problems • Ethical Committees open to research which seeks to tackle such problems
Regulatory issues • Regulatory bodies react to established procedures • Strong drive to classify work according to previous medical technologies-is it a device? –is it a medicine? • Tissue Engineering doesn’t fit either of above well and is being driven towards Medicinal Products • Running trials on autologous cell treatments not like drug development……not a great fit…
Regulatory issues • UK Regulatory bodies can be approached-you can get meetings –decisions are harder • Real need to work closely with MHRA and HTA to inform them of how fields are progressing
Economic issues • Products currently represent a small proportion of treatment cost • New technology will increase cost of product but reduce total cost to provider • Health economics are driving cure over treatment Cost of healing index Nursing time Products Other costs Source: Husing et al, 2003. The Future of Wound Care, MX (Market Analysis II) LEK Consulting, Feb 2006 Traditional Advanced Active Over 4 years
Summary Our philosophy of product development based on adult autologous cells is that these should be • Clinically effective • Low risk for the patient • Developed by working with clinicians and patients • Convenient to use –streamlined delivery We have developed a range of products and indications in the ‘active’ sector using autologous cells
Acknowledgements Grateful thanks to all those patients and clinicians who have worked with us to develop tissue engineered skin products for the treatment of burns and chronic wounds.