Download
1 / 56
570 likes | 967 Views
Descending and thoraco abdominal aortic aneurysms Kittichai Luengtaviboon M.D. 17 th september 2011. History of aortic surgery. 1950 Dubost French surgeon 1914-1991 resected ascending aortic aneurysm with end to end anastomosis.

E N D
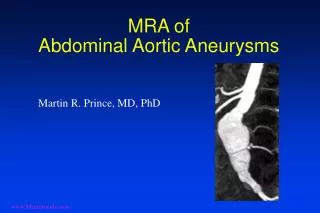
Descending and thoraco abdominal aortic aneurysmsKittichaiLuengtaviboon M.D.17thseptember 2011
History of aortic surgery • 1950 Dubost French surgeon 1914-1991 resected ascending aortic aneurysm with end to end anastomosis. • 1951 Dubost resected abdominal aortic aneurysm and replaced with homograft. • 1956 Dacron and teflon were used as aortic substitute. • The start of golden age of aortic surgery, Houston became the Mecca of aortic surgery.
1953 De Bakey used Dacron graft to treat descending thoracic aneurysm using Clamp and Go technique. • 1956 Houston group was the first to treat an aneurysm of the ascending aorta. • 1962 De Bakey published the results of a first series of 52 cases of aneurysms of the aortic arch. • 1963 De Bakey classification of aortic dissection. • 1970 Stanford classification.
Protection of viscera during descending aortic aneurysm repair • 1953 moderate hypothermia Hardin body surface hypothermia • 1957 Frank Gerbode – left heart bypass • 1963 Vincent Gott – shunt (heparin treated polyvinyl) • 1970 CM Dixon – Biomedicus pump • 1973 E Stanley Crawford – sequential aortic clamping in a caudal direction, • 1991 One year before his death, Crawford introduced a new classification of TAAA into 4 types.
1983 German surgeon- Hans George Borst proposed Elephant trunk technique. • 1988 use of CSF drainage to prevent paraplegia • 1992 Michael D. Dake (Stanford) used endograft to treat descending aneurysm. • 2000 French surgeon – EdouardKieffer proposed classification of descending aneurysm.
Classification of descending thoracic aortic aneurysms • Depend on extent of the aneurysm type A from LSCA to T6 type B from T6 to celiac A type C = A+B • Related to potential complications type A – stroke, hoarseness of voice type B – renal failure and paraplegia type C = all
etiology • Degenerative • Chronic aortic dissection • Inflammatory infected aortitis saccular form occur in region near visceral branches Takayasu’s disease
Indication for surgical management • Size • Growth rate • Symptoms • Etiology dissection infection
Technique of repair • Endovascular with hybrid arch coverage of celiac A LSCA coverage • Open repair
Open repair • Depend on type of DTA • Type A if unable to clamp distal to LCCCA – DHCA if clamp distal to LSCA is possible clamp and go distal adjunct left atriofemoral bypass femoro femoral bypass
Type B clamp and go with distal perfusion left atriofemoralbypasss femoro femoral bypass Gott’s shunt • Type C same as type A
151patients with DTA from 1989-2008 47% concurrent distal arch replacement Femoro femoral bypass Use thiopentone and methylprednisolone with head ice packing No cardioplegia, no monitoring of somato sensory and motor evoked potential Stop circulation after isoelectric EEG and nasopharyngeal temperature < 22 degree celcius
Thoraco abdominal aortic aneurysm • Definition – dilatation of aorta to a diameter at least 50% greater than expected normal diameter at diaphragmatic hiatus, with varying degrees of thoracic and abdominal extension. • Crawford’s classification risk stratification surgical approach select protective adjunct standarized reporting of results
3 major vascular units in Europe • 107 elective and urgent, high risk patients • All stents involved whole descending and abdominal aorta • Covered LSCA in 19, revascularization in 12 • Distal landing zone 75% infrarenal aorta, 25% iliac artery • 30 days mortality 14.95% • Spinal cord ischemia 12.1%, 8.4% complete and permanent • Long term dialysis 3.7% • Segmental bowel infarction 2.8% • 89 one stage 19 two stage
Endovascular treatment for TAAA • 50 years apart