Hypothesis
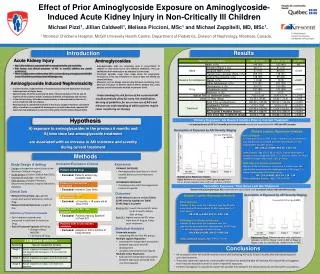
Effect of Prior Aminoglycoside Exposure on Aminoglycoside-Induced Acute Kidney Injury in Non-Critically Ill Children. Michael Pizzi 1 , Jillian Caldwell 1 , Melissa Piccioni , MSc 1 and Michael Zappitelli , MD, MSc 1.

Hypothesis
E N D
Presentation Transcript
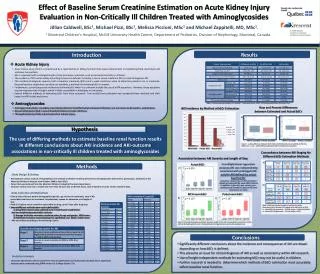
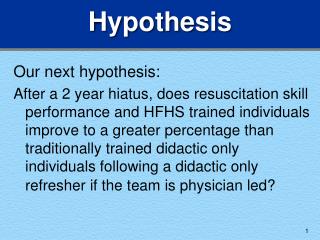
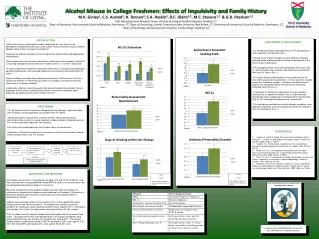
Effect of Prior Aminoglycoside Exposure on Aminoglycoside-Induced Acute Kidney Injury in Non-Critically Ill Children Michael Pizzi1, Jillian Caldwell1, Melissa Piccioni, MSc1 and Michael Zappitelli, MD, MSc1. 1Montreal Children’s Hospital, McGill University Health Centre, Department of Pediatrics, Division of Nephrology, Montreal, Canada. Results Introduction Acute Kidney Injury Aminoglycosides • AKI in ICU children is associated with increased mortality and morbidity. • Risk factors and clinical outcomes of AKI in non-ICU children are poorly understood. • There is single-centre evidence that AKI is common during aminoglycoside (AG) RX in non-ICU children and associated with longer stay. • Aminoglycosides (AG) are commonly used in non-critically ill children as they prove to be very effective antibiotics. They are administered intravenously or by nebulizer is some cases. • Treatment episodes range from single doses for prophylactic measures to 14-21 day treatments in cases of (but not limited to) severe infections. • Measures, such as dosage control using AG level monitoring, have been put into place to prevent adverse effects. Despite this, many patients are still dosed with multiple treatments of AG. Aminoglycoside Induced Nephrotoxicity • In animal studies, nephrotoxicity is characterized by renal cell dysfunction and acute tubular necrosis at higher doses. • Approximately 5% of the administered dose of AG accumulates in the S1 and S2 segment of the proximal tubule, leading to epithelial cell apoptosis and necrosis. • In the clinical setting, AG induced nephrotoxicity is characterized by slow rise in serum creatinine and non-oliguria. • Nephrotoxicity is considered reversible if the drug is stopped. However, cumulative effect of multiple or repeated AG treatments is not well understood; repeated AG exposures may predispose to recurrent ATN and/or chronic kidney disease (CKD). • Understanding the risk factors of AG-associated AKI would potentially allow for early risk stratification, devising of guidelines for use or non-use of AG’s and enhance our understanding of which patients require closer monitoring on therapy. Primary Exposure: AG Hours 6 months Prior to Current Treatment Hypothesis • Increasing hours of AG in 6 months prior to treatment was found associated with AKI and AKI severity. A) exposure to aminoglycosides in the previous 6 months and B) time since last aminoglycoside treatment are associated with an increase in AKI incidence and severity during current treatment Description of Exposure by AKI Severity Staging Multiple Logistic Regression Analysis One-way ANOVA test (p <0.0001) AKI as Outcome An increase in hours of AG in the 6 months prior to treatment was significantly associated with the development of AKI, independent of other factors. OR: 1.24, p <0.0001, 95% CI= 1.16-1.33 Other Factors: Age (OR: 0.96, p <0.05), Febrile Neutropenia relative to other diagnoses (OR: 1.72, p=0.01), Heme-onc Ward relative to surgery ward (OR: 2.60, p=0.001) AKIN Stage 2 or Greater as Outcome Higher number of AG hours in previous 6 months was also significantly associated with development of AKI Stage 2 or worse independent of all other factors OR: 1.24, p<0.001, 95% CI= 1.14- 1.34 Other Significant Factors: Age (0.94, p<0.005) Methods Inclusion/Exclusion Criteria Exposures Study Design & Setting • Design: retrospective cohort study at the Montreal Children’s Hospital • Study period: October 2008 to April 2012. • Inclusion & exclusion – see figure. • Data sources: Hospital Pharmacy Department database; hospital laboratory database. • PRIMARY EXPOSURE • Aminoglycosides (any) hours in the 6 months before current treatment episode SECONDARY EXPOSURE • Time(days) since LAST Aminoglycosidetreatment episode Multiple Linear Regression Analysis: Higher AG hours was associated with higher percent rise in SCr on therapy (adjusted beta-coefficient: +0.062, p<0.001) Secondary Exposure: Time Since Last AG Treatment • Shorter time from previous AG treatment was associated with increased risk for AKI and AKI severity. Clinical Data Outcomes Description of Exposure by AKI Severity Staging Multiple Logistic Regression Analysis • Relevant Clinical Data: Age, gender, reason and ward of admission, name of drug. • Relevant Clinical Outcomes: Length of stay. 1) AKI defined as yes or no (see Table) 2) AKI severity staging (see Table) 3) AKI Stage 2 or greater Baseline SCr: lowest measured SCr value up to 3 months before start of drug Peak SCr: highest measured SCr value from start of drug to 5 days post- treatment One-way ANOVA test (p <0.0001) AKI as Outcome Number of days since last treatment was significantly associated with development of AKI independent of other factors OR: 0.99, p=0.001, 95% CI= 0.99- 1.00 AKIN Stage 2 or Greater as Outcome Number of days since last treatment was also significantly associated with development of AKI Stage 2 or worse independent of other factors OR: 0.99, p=0.035, 95% CI= 0.99-1.00 Other Significant Factors: Age (0.94, p=0.014) Definition of Treatment Episode • Each treatment episode was measured in total time (in hours) on Drug • End of Treatment Episode defined by • Change of drug AND/OR • > 24 hours off drug Statistical Analysis • Univariateanalysis • comparing AKI and non AKI groups. • Multiple Logistic Regression • assessing the independent association between exposures and AKI development • variables controlled for (see figure) • Multiple Linear Regression • Evaluate the independent association between exposures and peak %SCr • rise from baseline Bonferroni Test: Differences were only significant between no AKI vs Stage 1 and no AKI vs Stage 2. Stage 3 was not significantly different from no AKI. Conclusions • An increased risk for AKI and AKI severity is seen with increasing AG hours in last 6 months and with decreasing time since last treatment. • These may represent important, ascertainable risk factors for predicting who will develop AG-induced AKI and suggests that it may be desirable to avoid or control repeat AG exposures. • Further investigation is required to explore the possible links between the above exposures and biomarker associations.