Download
1 / 20
720 likes | 6.41k Views
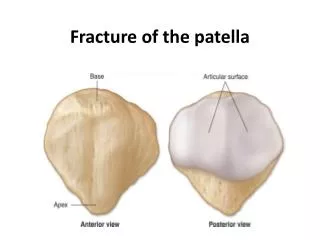
Fracture of the patella. Cont. Fig . Anatomy. Largest sesamoid bone in the body. Quadriceps tendon inserted on the superior pole and the patellar ligament originates from the inferior pole. Funtion of the patella is to increase the mechanical advantage and protection. Cont. Fig .

E N D
Cont.. • Fig
Anatomy • Largest sesamoid bone in the body. • Quadriceps tendon inserted on the superior pole and the patellar ligament originates from the inferior pole. • Funtion of the patella is to increase the mechanical advantage and protection.
Cont.. • Fig
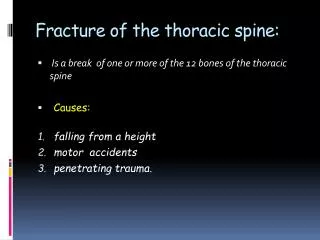
Mechanism of injury Direct trauma : • Due to direct fall over the patella • Usually cause comminuted fractures and are the common causes Indirect trauma (quadriceps contraction ): • Sudden forceful contraction of the quadriceps (as in sports ) • Age : common in 20 – 50 years age group
Clinical evaluation- • Patient usually non ambulatory. • Pain, swelling • Abrasion over the patella. • Unable to extend the knee • Both the active and passive movements are restricted
On examination • Palpable gap • Tenderness • signs of effusion • Positive patellar
Classification Undisplaced • Transverse fracture (80%) • Vertical fracture • Comminuted fracture Displaced Transverse (85 %) • Oblique fracture • Vertical fracture • Comminuted fracture osteochondral fracture
Classification • Fig
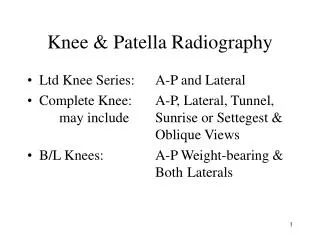
Investigation X – ray : • AP view • lateral view • Skyline view • CT scan • Bone scan • MRI
Lateral view • Fig :
Skyline view • Fig
Tests : • Patellar tap • Fluctuation test
Patellar tapping • Fig :
Treatment • Non operative • For non displaced fracture • Cylinder cast: extending from the groin to just above the malleoli for 4 to 6 weeks. • Followed by physiotherapy- quadriceps strengthening exercise.
Operative- • Tension band wiring. (figure of 8) • Patellectomy • Partial:for proximal pole fracture; major fragment is preserved;. • Complete: for comminuted fractures. • Knee should be immobilized for 3 to 6 weeks in a long leg cast at 10degrees flexion for both partial and complete patellectomy.
Patella Knee Support • Fig
Cont.. • Open reduction and internal fixation for transverse fracture
Complications • Refracture • Non union • Avascular necrosis of fragments • Osteoarthritis • Knee stiffness • Patellar instability