Download
1 / 66
720 likes | 835 Views
Learn about leukoplakia, erythroplakia, oral submucous fibrosis, lichen planus, Plummer Vinson syndrome, and more. Find out about symptoms, diagnosis, and management of these premalignant lesions.

E N D
PREMALIGNANT LESIONS • Leukoplakia • Erythroplakia • Oral submucous fibrosis • Lichen planus • Plummer Vinson syndrome • Syphilis
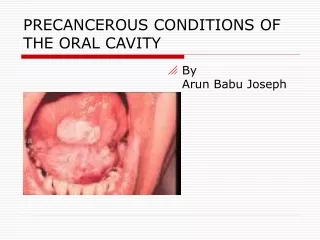
LEUKOPLAKIA • Definition:A clinical white patch that cannot be characterised clinically or pathologically as any other disease. • Aetiology: Smoking, tobacco chewing, alcohol, chronic trauma, ill fitting dentures • May be associated with submucous fibrosis, hyperplastic candidiasis or PV syndrome
LEUKOPLAKIA • Sites: Buccal mucosa, oral commissure, floor of the mouth, tongue, GB sulcus, lips • 4th decade, M:F – 3:1 • D/D: D/D-white lesions- lichen planus, discoid lupus erythematosis, white spongy nevus, candidiasis • Types: • Amorphous – smooth, white patch • Speckled – nodular with erythematous base • Erosive – has erosions and fissure, more likely to turn malignant
Histology: 25% show evidence of dysplasia 1-17.5% can turn malignant Management: Treat the cause Biopsy to rule out malignancy Excision with laser LEUKOPLAKIA
ERYTHROPLAKIA • A red lesion on the mucosal surface that cannot be characterised as another entity. • Red colour is due to reduced keratinisation because of which the red vascular connective tissue of the submucosa shines through.
Sites: Lower alveolar mucosa, GB sulcus, floor of the mouth HPE; severe dysplasia, ca in situ, frank malignancy Malignant potential is 17 times higher than leukoplakia ERYTHROPLAKIA
ERYTHROPLAKIA • Types: • Homogenous • Speckled • Granular • Erthroplakia interspersed with leukoplakia • Treatment: • Excision and follow up
Oral lichen planus • 0.2%- 2% of the population is affected • Usually asymptomatic, reticular form, white lace like symmetric lesions in the buccal mucosa • T-cell lymphocytic reaction to antigenic components in the surface epithelial layer • Other variants: plaque, atrophic/erythematous, erosive
Oral submucous fibrosis Progressive fibrosis of the oral cavity of unknown aetiology characterised by juxtaepithelial deposition of fibrous tissue First described by Joshi 1953 29 October 2019 14
Aetiology Prolonged irritation due to tobacco, betel nuts, lime, chillies, alcohol Auto immune disease affecting collagen Deficiency of vitamin A & B complex Multifactorial 29 October 2019 15
Pathogenesis HPE: Early stages – Infiltration with neutrophils, eosinophils & few lymphocytes, Late stages – More of lymphocytes & plasma cells with fibrosis High T lymphocytes, less of B cells & macrophages High CD4+ to CD8+ Lymphocyte ratio Loss of vascularity in lamina propria, submucosa & muscles Production of cytokines which act on mesenchymal cells to produce fibrosis & cause down regulation of collagenase production and increased collagen production 29 October 2019 17
Pathology Fibroelastotic transformation of connective tissue in lamina propria Epithelial atrophy Vesicle formation Progressive trismus May predispose to leukoplakia and squamous cell carcinoma Premalignant condition 3-8% 29 October 2019 18
Clinical features 20-40 years, both the sexes Symptoms: Intolerance to hot & spicy food, burning sensation in mouth, Difficulty in opening the mouth & difficulty in tongue protrusion Signs: Fibrotic changes over soft palate, faucial pillars & buccal mucosa restricting the mobility of the palate, tongue & jaw Vesicles in early stages, fibrosis in late stages Progressive trismus, poor orodental hygiene 29 October 2019 19
Treatment - Medical Steroids – Topical dexamethasone with hyalase (4 mg with 1500 IU) biweekly for 8-10 weeks Avoid irritants Treat anaemia/vitamin deficiency Jaw opening exercises Antioxidants 29 October 2019 20
Treatment - Surgical Release of fibrosis with laser & skin grafting Tongue/nasolabial flaps Palatal mucoperiosteal flaps Radial forearm free flaps Excision & buccal fat pad graft Temporalis fascia & skin graft Coronoidectomy & temporal muscle myotomy 29 October 2019 21
Plummer Vinson Syndrome • Patterson Brown Kelly Syndrome • Dysphagia, Iron deficiency anaemia, glossitis, angular stomatitis, kolionychia & achlorohydria • Females,> 40 years • Ba swallow; web in post cricoid region • 10% can develop post cricoid carcinoma • Also predisposes to other upper aerodigestive malignancies • Treatment: Correction of anaemia, dilatation of web
MALIGNANCY OF THE ORAL CAVITY • 3-4% of all the cancers • 96% are carcinomas and 4% are sarcomas • 90% are squamous cell carcinomas • >10000 people die every year because of oral cancer • <50% survive for 5 years after the diagnosis
Mucosal lip Buccal mucosa Oral Tongue – most common Hard palate Upper & lower alveolar ridges Floor of the mouth RMT SITES
AETIOLOGY • Tobacco smoking & chewing • Alcohol • Age: > 40 years • M:F – 6:1 • Race: Black: White – 2:1 • ?Sunlight – lips • HPV 16 &18 • Dietary deficiency of vit B2, B12, Carotenoids • Premalignant lesions – Leukoplakia, erythroplakia, OSMF etc • 6 ‘S’: Smoking, Spices, Sepsis, Spirit, Sharp tooth, Syphilis
PATHOLOGY • Gross: • Proliferative • Ulcerative • Ulceroproliferative • Infiltrative • Microscopy: • Sq cell ca: Epithelial pearls & clusters of squamous cells with varying degrees of differentiation, occasionally verrucous carcinoma with keratinisation
SPREAD • 15% can have multiple primaries • Local: • Into the submucosa, muscle, fat, skin, mandible and adjacent regions • Lymphatic: • Bilateral or contralateral nodal involvement, Level 1 & 2 nodes • Distant: • Rare.
CLINICAL FEATURES - SYMPTOMS • Asymptomatic initially • Burning sensation in the mouth • Discomfort, numbness over the site of the lesion • Loose teeth or ill fitting dentures • Increased salivation • Difficulty in mastication • Dysphagia/odynophagia • Mass in the oral cavity • Referred ear pain • Cheek swelling or ulceration • Neck swellings
CLINICAL FEATURES - SIGNS • Ulceroprolifeartive growth – site & extent needs to be noted • Associated leukoplakia or erythroplakia or OSMF • Mandibular involvement – thickening, tenderness • Tongue movements may be restricted • Cervical lymph nodes – level 1 & 2 may be palpable
INVESTIGATIONS • Biopsy: punch/wedge biopsy from the margins • FNAC of the lymph nodes • X-Ray of the mandible/OPG/CT Scan • Chest X-ray
TREATMENT • Options available: • Surgery • Radiotherapy • Chemotherapy
SURGERY • Wide excision with at least 1.5-2 cm margin of the normal tissue all around along with extended supra omohyoid dissection. Most often for stage 2, 3 &4 if operable, often combined with RT • Mandible: Segmental/marginal/hemi/mandibulotomy for access • Reconstruction: Primary/local/myocutaneous/free flaps
RADIOTHERAPY • For stage 1, occassionally stage 2 lesions as the primary modality, otherwise combined with surgery or chemotherapy • Risk of osteo radio necrosis • Teletherapy: • 6800 rads in 28 - 30 fractions over 5 weeks • Brachytherapy: • Using needles/seeds/wires of iridium 192, celsium, pallidium
CHEMOTHERAPY • Adjuvant only • Occasionally as palliative • Ciplatinum, 5FU & methotrexate
Malignancy Lip • SCC, males 40-70yrs, lower lip (between midline and commissure of lip) • Exophytic or ulcerative • LN mets late- submental or submandibular-deep cervical nodes • Rx- wide surgical excision and repair of defect. Lymph node - neck dissection • Or Radiotherapy 25
Malignancy buccal mucosa • Very common- seen in both sexes • Most common-angle of mouth or line of occlusion of upper and lower teeth; buccal sulcus where tobacco quid is kept- multicenteric foci • Exophytic or ulceroinfiltrative • Common site for verrucous ca 27
• Spread- deeper- submucosa-muscle-subcutaneous fat-skin. — Muscle-buccinator or masseter-trismus — Anteriorly - angle of mouth & lip. — Posteriorly - retromolar trigone & med pterygoid M. — Superiorly - upper GB sulcus & maxilla. — Inferiorly - lower GB sulcus & alveolar margin 29
• LN- 50% - submandibular and upper jugular nodes • Early cases- asymptomatic; pain and bleeding in mouth as ulcerates and invades deeper • Involvement of buccinator, masseter / pterygoid muscles - trismus • Foul smelling bleeding mass - later features 30
Treatment • T1N0- surgical excision and follow up • T2N0- no bone involved- radiotherapy to growth and lymph node • Bone involved- surgery- excise growth and reconstruction of area 31
• Higher stages- surgical resection, reconstruction with skin / myocutaneous flaps and post-op radiotherapy. Neck dissection of palpable lymph nodes 32
Anterior 2/3rd tongue • Men-50-70yrs • Rarely in younger age and females • Pre-existing leukoplakia, chronic dental ulcer, syphilitic glossitis • Squamous cell ca • Most - middle of lateral border or ventral aspect of tongue, rarely tip or dorsum involved 33
• Spread-locally-infiltrate deeply into musculature-restrict movements — Spread to floor of mouth, alveolus, mandible • LN - lateral border of tongue - submandibular and upper jugular — Tip - submental and jugulo-omohyoid — Unilateral or bilateral 34
• Appearance- exophytic lesion like papilloma • Non-healing ulcer with rolled edges, greyish white shaggy base and induration • Submucous nodule with induration of surrounding tissue 35
Clinical features • H/o-early stage-painless and asymptomatic • Pain at site of ulcer, burning sensation • Pain in ipsilateral ear-nerve supply (mandibular nerve)-advanced stage • Swelling in mouth 37