Download
1 / 17
170 likes | 254 Views
Explore Delaware's homeless assistance system data, funding sources, and program implementation experiences, with a focus on effective planning and assessment strategies for homelessness prevention and rapid re-housing. Discover insights, challenges, and outcomes from Delaware's continuum of care initiatives.

E N D
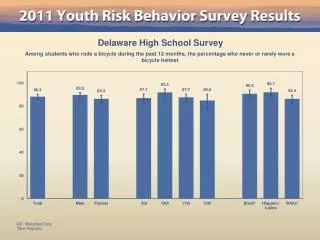
Effective Use of Homeless Program Data: Delaware’s Experience COSCDA 2011 Annual Training Conference September 20, 2011 Susan Starrett (302) 654-0126 sstarrett@hpcdelaware.org www.hpcdelaware.org
Delaware in a Nutshell Small BUT Mighty!
Delaware’s Homeless Assistance System • ~ 1,500 people homeless during any given night • ~6,500 people homeless each year • 41 Agencies102 Programs1,960 Total Beds • 670 Emergency Shelter Beds • 890 Transitional Housing Beds • 400 Permanent Supportive Housing Beds • 10 Year Plan to End Chronic Homelessness and Reduce Long-term Homelessness • Approved in February 2007 • Need: 2,003 Beds • Expected Progress by December 2011: 551 Beds
Funding for Homelessness in DE • $19,956,020 supports all emergency, transitional and permanent supportive housing programs • 52% from Federal Resources • 33% from Local Government and Private Resources • 15% from State Resources • DE does not have a unit of state government responsible for homelessness • All state resources either come through Grant-in-Aid or through non-homeless housing and service departments • 5 Housing Jurisdictions (4 Consolidated Plans) • 3 Entitlement Housing Jurisdictions Data from a DSHA 2006 Survey
DE’s Continuum of Care • Delaware has a statewide Continuum of Care • In 1998, Homeless Planning Council of DE was created to serve as Continuum of Care Lead Agency and Planning Body • Began conducting PIT Surveys and Needs Assessments in 2001 • In 2004, HPC took over as System Administrator for DE’s statewide implementation of HMIS • In 2005, Delaware Interagency Council on Homelessness was created by Executive Order (codified in 2009)
HMIS Implementation • Statewide • Started with 6 providers – now 22/39 agencies participate • In 2008, started sharing First Name, Last Name and SSN • Agencies and Clients decide how much other data to share • Expansion to Non-Homeless Service Providers (Financial Empowerment Centers, Community Reinvestment Action Council, Re-entry Community, Health and Social Services, Libraries/Job Centers, etc.)
HPRP Implementation and Assessment Planning for change when things need to be implemented yesterday!
Planning for HPRP Implementation • Pre-ARRA: • Delaware had Cash Financial Assistance programs that serve people in poverty • Delaware had no coordinated, targeted homeless prevention programs • Rapid Re-Housing was something we heard about at National Conferences, but no discussion of implementing in Delaware • ARRA signed into law with 90 days to amend Consolidated Plans • 90 days to create a Homeless Prevention and Rapid Re-Housing System among 3 entitlement jurisdictions
Planning for HPRP Implementation (cont.) • HPC contacted all 3 jurisdictions and asked for a joint meeting • Discussed how to: • Create a Homeless Prevention and Rapid Re-Housing Program • Create 1 Statewide RFP, so agencies didn’t have to apply to all 3 jurisdictions and funding decisions could be made together • Use HMIS for Eligibility Determination Screening • In August 2009, began coordinating with DSS and 3 jurisdictions about use of TANF-ARRA dollars for HPRP
HPRP Implementation • $3M HPRP (3 jurisdictions) plus $5M TANF funds • All funds tracked in HMIS • HMIS used for Eligibility Determination Screening • CBO’s conducted intakes • CBO’s inputted intake info into HMIS • HPC reviewed intake info to ensure eligibility and non-duplication of services across jurisdictions and gave final approval • Eligibility Determination Form
HPRP Assessment • Not all poor people become homeless…and not all people who are cost-burdened or severely cost-burdened become homeless… so who does become homeless and how do we target resources to best prevent them from becoming homeless? • Program Design: Followed HUD’s recommendations for persons most at-risk of homelessness – was that enough?
Homeless Population Comparisons November 1, 2009 – September 30, 2010HPRP and TANF Funds (N=4,477) July 1, 2009 – June 30, 2010HMIS Participating Homeless Providers (N=3,147) Homeless Prevention
Homeless Population Comparisons November 1, 2009 – September 30, 2010HPRP and TANF Funds July 1, 2009 – June 30, 2010HMIS Participating Homeless Providers Homeless Prevention
Homeless Population Comparisons November 1, 2009 – September 30, 2010HPRP and TANF Funds July 1, 2009 – June 30, 2010HMIS Participating Homeless Providers Homeless Prevention
Prevention Homeless Legend Legend 0.027144% - 3.224756% 0.040355% - 3.46247% 3.224757% - 6.422367% 3.462471% - 6.884584% 6.422368% - 9.619978% 6.884585% - 10.306699% 9.619979% - 12.81759% 10.3067% - 13.728814% 12.817591% - 16.015201% 13.728815% - 17.150928%
Now that we know this… • We need to continue collaborating and designing programs together • We need to design a prevention program that does a better job targeting resources • We need a centralized system of determining eligibility for programs • Prevention • Diversion • Centralized Intake • We need to include all stakeholders, not just the ‘usual’ ones (churches, state government, local governments, community groups, etc.)