Download
1 / 48
640 likes | 2.86k Views
ANTICOAGULATION in CRRT: Heparin vs. Citrate. Patrick D Brophy MD Pediatric Nephrology CS Mott Children’s Hopsital University of Michigan. Outline. Normal Coagulation Cascade Anticoagulation: Options Heparin Citrate Others Literature & conclusions. Normal Coagulation.

E N D
ANTICOAGULATION in CRRT:Heparin vs. Citrate Patrick D Brophy MD Pediatric Nephrology CS Mott Children’s Hopsital University of Michigan
Outline Normal Coagulation Cascade Anticoagulation: Options Heparin Citrate Others Literature & conclusions
Normal Coagulation Tissue Factor (extrinsic) TF:VIIa Contact Phase (intrinsic) XII activation XI IX platelets / monocytes / macrophages X Xa Va VIIIa Ca++ platelets prothrombin THROMBIN fibrinogen CLOT
Any blood surface interface Hemofilter Bubble trap Catheter (Especially Pediatrics) Areas of turbulence resistance Luer lock connections / 3 way stopcocks Sites of Thrombus Formation
No anticoagulation Technical aspects cannulation / circuit Blood flow rate FF / predilution Saline flush Hemodilution Heparin Unfractionated LMWH Citrate Others Prostacyclin Danaparoid Hirudin Anticoagulation: Options
Saline Flushes Heparin: systemic, regional (?) Citrate regional anticoagulation Low molecular weight heparin Prostacyclin Nafamostat mesilate Danaparoid* Hirudin/Lepirudin Argatroban (thrombin inhibitor)* Anticoagulants * No antidote known
Can you run anticoagulation free? Having no anticoagulation shortens circuit life Will you use Heparin? What is the risk on Patient bleeding Platelet count (HIT) Will you use Citrate? What is the risk on Patient calcium Anti-Coagulation
Sites of Action of Heparin Contact Phase (intrinsic) XII activation XI IX Tissue Factor (extrinsic) TF:VIIa platelets / monocytes / macrophages X Xa Va VIIIa Ca++ platelets LMWH UF HEPARIN prothrombin THROMBIN fibrinogen CLOT
No Heparin Systemically Heparinized NO surface - no heparin NO surface - heparinized
Reduced risk of bleeding Less risk of HIT LMWH: Theoretic advantages
No difference in risk of bleeding No quick antidote Increased cost No difference in filter life LMWH
Heparin infusion prior to filter with post filter ACT measurement and heparin adjustment based upon parameters Bolus with 10-20 units/kg Infuse heparin at 10-20 units/kg/hr Adjust post filter ACT 180-200 secs Interval of checking is local standard and varies from 1-4 hr increments Heparin Protocols
Benefits Heparin infusion prior to filter with post filter ACT measurement Bolus with 10-20 units/kg Infuse at 10-20 units/kg/hr Adjust post filter ACT 180-200 secs Risks Patient Bleeding Unable to inhibit clot bound thrombin Ongoing thrombin generation Activates - damages platelets / thrombocytopenia Heparin Protocols Benefit and Risks
How does it work? Is there an advantage over heparin? What are the side effects? How easy is it to use? What are the protocols? What is needed to make it work Citrate anticoagulation
Citrate anticoagulation with CRRT (Regional citrate anticoagulation for CAVHD in critically ill patients. Kidney Int 38; 976-978, 1990. RL Mehta) n = 18 2652 hr CAVHD filter survival trended longer with citrate n = 3, metabolic alkalosis Rx iv HCl n = 1, hypernatremia Background:
Complications of citrate protocols: “The potential complications Hypocalcemia Hypercalcemia Hypernatremia Metabolic alkalosis have generally made this regimen less desirable than minimal dose heparin” Need for Designer Solutions Method of measuring anticoagulation efficacy What has limited citrate use in the past: E.C. Kovalik. UpToDate. Hemodialysis anticoagulation, October 19, 2000
Clotting is a calcium dependent mechanism, removal of calcium from the blood will inhibit clotting Adding citrate to blood will bind the free calcium (ionized) calcium in the blood thus inhibiting clotting Common example of this is blood banked blood How does citrate work
Ca++ Ca++ Ca++ Ca++ Ca++ Ca++ Sites of Action of Citrate TISSUE FACTOR TF:VIIa CONTACT PHASE XII activation XI IX monocytes / platelets / macrophages X Va VIIIa Ca++ platelets Xa Phospholipid surface prothrombin CITRATE THROMBIN NATURAL ANTICOAGULANTS (APC, ATIII) FIBRINOLYSIS ACTIVATION FIBRINOLYSIS INHIBITION fibrinogen CLOT
Unclear from literature Pediatric clinical experience Animal study: initial citrate flow rates Require a citrate concentration ~ 6mmol/L to achieve iCa++ < 0.4mmol/L Qc x Cc Qb + Qc + QR Pre-filter [citrate] = Citrate: Pediatric Dosage Qc = citrate flow Cc = citrate concentration Qb = blood flow rate QR = replacement fluid flow rate
Binds calcium - essential co-factor Citrate: Mechanism of Action
In most protocols citrate is infused post patient but prefilter often at the “arterial” access of the dual (or triple) lumen access that is used for hemofiltration (HF) Calcium is returned to the patient independent of the dual lumen HF access or can be infused via the 3rd lumen of the triple lumen access How is citrate used?
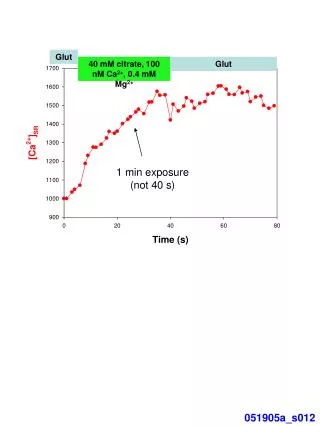
(1.5 x BFR) (0.4 x citrate rate)
Measure patient and system iCa in 2 hours then at 6 hr increments Pre-filter infusion of Citrate Aim for system iCa of 0.3-0.4 mmol/l Adjust for levels Systemic calcium infusion Aim for patient iCa of 1.1-1.3 mmol/l Adjust for levels Citrate: Technical Considerations
No need for heparin Commercially available solutions exist (ACD-citrate-Baxter) Less bleeding risk Simple to monitor Many protocols exist Citrate: Advantages
Has zero effect upon patient bleeding as opposed to heparin which effects system and patient bleeding Easy to monitor with ionized calcium assay Activated Clotting Time (ACT) nor PTT needed Programs report less clotted circuits = less disposable cost and less overtime nursing hours Bedside surveys demonstrate less work of machinery allowing more attention to patient Advantages of Citrate
Metabolic alkalosis Metabolized in liver / other tissues Electrolyte disorders Hypernatremia Hypocalcemia Hypomagnesemia Cardiac toxicity Neonatal hearts Citrate: Problems
Metabolic alkalosis due to citrate conversion to HCO3 Solutions with 35 meq/l HCO3 NG losses TPN with acetate component Complications of Citrate:Metabolic alkalosis
Rx Metabolic alkalosis by Solutions with 35 meq/l HCO3 Decrease bicarbonate dialysis rate and replace at the same rate with NS (pH 5) to allow for the total solution exposure to be identical (ie no change in solute clearance) yet this will give less HCO3 exposure and an acid replacement NG losses Replace with ½-2/3 NS TPN with acetate component Use high Cl ratio Complications of Citrate:Rx of Metabolic alkalosis
Seen with rising total calcium with dropping patient ionized calcium Essentially delivery of citrate exceeds hepatic metabolism and CRRT clearance Rx of “citrate lock” Decrease or stop citrate for 3-4 hrs then restart at 70% of prior rate Complications of Citrate: “Citrate Lock”
Frequent clotting is a vascular access problem. High flow CVVHDF is more effective at clearing citrate from circulation….keep dialysate + replacement = 40 – 50 ml/min/1.73 m2 Keep circuit [Ca++] levels around .30 for best results. Lock catheter with tPA between every circuit change. Citrate Pearls
Citrate Hoffbauer R et al. Kidney Int. 1999;56:1578-1583.
Unfractionated Heparin Hoffbauer R et al. Kidney Int. 1999;56:1578-1583.
single center analysis in 209 adults regional anticoagulation with trisodium citrate in combination with a customized calcium-free dialysate was utilized in comparison to a standard heparin protocol. CitACG was the sole anticoagulant in 37 patients, 87 patients received low-dose heparin plus citrate, and 85 patients received only hepACG. Both groups receiving citACG had prolonged filter life when compared to the hepACG group. complications included; metabolic alkalosis (50% of patients on citACG), alkalosis (resolved by increasing the dialysate flow rate) and hypercalcemia. This study also demonstrated a significant cost saving due to prolonged filter life when using citACG. Heparin or Citrate?. Morgera S, et.al. Nephron Clin Pract. 2004; 97(4):c131-6.
39 children with CRRT from 1995-1999 System Gambro PRISMA 13 patients underwent heparin anticoagulation 16 patients underwent citrate anticoagulation Heparin or Citrate?(M Golberg RN et al, Edmonton pCRRT 2002)
Heparin circuits 13 patients with 45 filters 29.4 + 23 hrs average length of circuit Citrate circuits 16 patients with 51 filters 49.1 + 26 hrs average length of circuit (p < 0.001) Heparin or Citrate?
Brophy et.al. NDT 2005 Jul;20(7):1416-21 Comparison of CRRT circuit life for all circuits with: no anticoagulation (filled squares), heparin anticoagulation (filled circles) or citrate anticoagulation (filled triangles). Mean circuit survival was no different for circuits receiving hepACG (42.1±27.1 h) and citACG (44.7±35.9 h), but was significantly lower for circuits with noACG (27.2±21.5 h, P<0.005).
Brophy et.al. NDT 2005 Jul;20(7):1416-21 Comparison of CRRT circuit life for PRISMA circuits with: no anticoagulation (filled squares), heparin anticoagulation (filled circles) or citrate anticoagulation (filled triangles). Mean circuit survival was no different for circuits receiving hepACG and citACG but was significantly lower for circuits with noACG (P<0.005).
Regional Anticoagulation No systemic anticoagulation effect Can be used in patients with HIT Prolongs Filter Life Why I feel citrate is superior to systemic Heparinization
Web Sites: WWW.PCRRT.COM Pioneering work: adults– Mehta, Gibney, Tobe, Niles Bunchman Protocols for Citrate anticoagulation
All commercially available solutions Citrate Regional Anticoagulation Minimal Set up/Pharmacy involvement Regulates/Nursing Algorithms: Clearance Citrate monitoring (post filter iCa) Calcium Monitoring Acid/Base balance Volume/electrolyte Ideal Setup for CRRT
ppCRRT group Dr. Stu Goldstein (TCH)/Dr. Peter Skippen (BC Children’s Hospital) Theresa Mottes Hemodialysis Staff Organizers for such a wonderful meeting! Final Thoughts