SPARLON™ (modafinil) Tablets [C-IV]
1.19k likes | 1.52k Views
SPARLON™ (modafinil) Tablets [C-IV]. Psychopharmacologic Drugs Advisory Committee 23 March 2006. Introduction. Victor Raczkowski, M.D., M.S. VP, Worldwide Regulatory Affairs Cephalon, Inc. SPARLON Tablets. Proposed Indication

SPARLON™ (modafinil) Tablets [C-IV]
E N D
Presentation Transcript
SPARLON™ (modafinil) Tablets [C-IV] Psychopharmacologic Drugs Advisory Committee 23 March 2006
Introduction Victor Raczkowski, M.D., M.S. VP, Worldwide Regulatory Affairs Cephalon, Inc.
SPARLON Tablets • Proposed Indication Treatment of Attention Deficit Hyperactivity Disorder (ADHD) in children and adolescents • Regulatory Status • Filing: 20 Dec 2004 • Approvable Letter: 20 Oct 2005 • Complete response: 21 Nov 2005
SPARLON Formulation • Modafinil is the active ingredient in SPARLON, the same as in PROVIGIL® Tablets • Smaller than PROVIGIL Tablets and film-coated • Dosage strengths of 85, 170, 255, 340, & 425 mg
PROVIGIL® (modafinil) Tablets [C-IV] • Marketed in the US since 1999 and in 28 countries worldwide • US approval in adults with excessive sleepiness: • narcolepsy • obstructive sleep apnea / hypopnea syndrome • shift work sleep disorder • Exposure: 780,000 patient-treatment years • Adults: 750,000 patient-treatment years • Pediatrics: 30,000 patient-treatment years • Modafinil: Schedule IV of the Controlled Substances Act
Overview • SPARLON has been shown to be effective for the treatment of ADHD in pediatric patients • SPARLON has been shown to be acceptably safe in the treatment of ADHD in pediatric patients • The Benefit-Risk profile of SPARLON in the treatment of ADHD in pediatric patients is favorable
Modafinil and Pediatric Stevens Johnson Syndrome (SJS) • Pediatric Clinical Trials • 1 case of probable SJS • Uncertain etiology • 1622 patients • Pediatric Postmarketing Experience • No cases • 30,000 pediatric patient-treatment years
Psychiatry/ADHD Joseph Biederman, M.D.* Samuel Boellner, M.D.* Thomas Spencer, M.D.* Sharon Wigal, Ph.D.* Dermatology Amy Paller, M.D. Neil Shear, M.D. Addiction Medicine Charles Dackis, M.D. Cardiology Craig Pratt, M.D. Jonathan Sackner-Bernstein, M.D. Child Development Thomas Rugino, M.D.* James Swanson, Ph.D.* Epidemiology Greg Burkhart, M.D. John Clark, M.D. Joel Gelfand, M.D. Consultants *Investigator in ADHD Clinical Studies
ADHD as a Lifelong Brain Disorder of Genetic Etiology and Poor Prognosis Joseph Biederman, M.D. Professor of Psychiatry, Massachusetts General Hospital and Harvard Medical School
Genetic origins NeuroanatomicNeurochemical ADHD • CNS insults • Environmental factors ADHD:Etiology ADHD is a heterogeneous behavioral disorder with multiple possible etiologies
ADHD:Worldwide Prevalence in School Age Children Site, Year Criteria Prevalence Faraone et al (2003). World Psychiatry, 2, 104-113
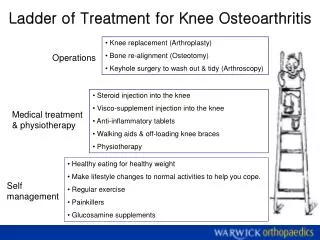
Developmental Trajectories of Brain Volume Abnormalities in Youth w/ADHD • Design: MRI case control study • N=152 youth w/ ADHD and 139 controls of both genders • Objective: assess volumetric changes overtime in medicated vs unmedicated youth w/ADHD and controls Castellanos et al. JAMA. 2002 Oct;288(14):1740-8
Developmental Trajectories of Brain Volume Abnormalities in Youth w/ADHD • Main Findings: • Smaller brain volumes in all regions independently of medication status • Smaller total cerebral (-3.2%) and cerebellar (-3.5%) volumes • Volumetric abnormalities (except caudate) persisted with age • No gender differences • Volumetric findings correlated with severity of ADHD Castellanos et al. JAMA. 2002 Oct;288(14):1740-8
1150 1050 950 850 5 10 15 20 Developmental Trajectories of Brain Volumes mL NV Males ADHD Males NV Females ADHD Females Age (y) Castellanos et al. JAMA. 2002 Oct;288(14):1740-8 From: http://www.nimh.nih.gov/events/pradhdmri.cfm
Developmental Trajectories of Brain Volume Abnormalities in Youth w/ADHD • Conclusions: • Genetic and or early environmental influences on brain development in ADHD are fixed, nonprogressive and unrelated to stimulant treatment Castellanos et al. JAMA. 2002 Oct;288(14):1740-8
ADHD:Neurobiologic Basis Attention Networks Executive Control Orienting (Selective Attention) Alerting Posner and Raichle. Images of Mind. Scientific American Books; 1996.
Smaller Dorsal and Rostral ACC in ADHD Seidman et al.
Cerebral Cortex Cortical Volume Cortical Thickness Vogt, 2005
Supramarginal Gyrus • (BA 40) • Dorsolateral Frontal Cortex (BA 8, 9) • Angular Gyrus • (BA 39) • Anterior Cingulate Gyrus (BA 24) • Middle Temporal Gyrus • (BA 21) • Superior Temporal Gyrus • (BA 22)
Diffusion Tensor MRI Fractional Anisotropy (FA) differences between normal controls and adults with ADHD overlayed onto a parasagittal T2 anatomical template Corpus callosum (body) dACG white matter Perigenual ACG white matter Corpus callosum (genu) Anterior Cingulate (ACG) gyrus white matter fractional anisotropy (FA) decrease in adults with ADHD. Alteration of anatomic connections is suggested on the perigenual and dorsal (dACG) anterior cingulate white matter region in adults with ADHD
Normal Controls ADHD y = +21 mm y = +21 mm -2 1 x 10 1 x 10 -2 1 x 10 -3 1 x 10 -3 MGH-NMR Center & Harvard- MIT CITP Bush et al, Biological Psychiatry 1999 Dorsal Anterior Cingulate Cortex (Cognitive Division) Fails to Activate in ADHD
Toward a Dual Pathway Model Directed Attention Fascination Executive circuit • Inhibitory deficits • Executive dysfunction Reward circuit • Reduce time to reward • Delay aversion ADHD Sonuga-Barke. Neurosci Biobehav Rev. 2003;27:593.
Twin Studies ADHD: Genetics Family Studies Genetic Basis of ADHD Adoption Studies Molecular Genetics
Schizophrenia Panic Disorder Height Mean Heritability=.77
ADHD:Molecular Genetics • Specific genes associated with ADHD • rare mutations in the human thyroid receptor- gene on chromosome 3 • dopamine transporter gene (DAT1) on chromosome 5 • dopamine receptor D4 gene (DRD4) on chromosome 11 Hauser et al. N Engl J Med 1993;328:997. Gill et al. Mol Psychiatry 1997;2:311. Swanson et al. Mol Psychiatry 1998;3:38.
Pooled Odds Ratios from Positive Meta Analyses (Faraone et al., Biological Psychiatry, in press)
Medication management + behavioral treatment Medication management alone Nearly equally effective and superior to both: ADHD: MTA Results All treatment arms found to be effective on an absolute basis • Behavioral treatment alone • Community based treatment MTA Study Group, Arch Gen Psych, 1999 Dec;56(12):1073-86
Long-Term Outcomes of Therapies for ADHD in the MTA Study Hyperactive Impulsive Symptoms (Teacher Reports) 70 60% 56% 60 50 45% 40 36% Improvement at 14 months (%) 30 20 10 0 Medication Combination Behavioral Community-based management therapy treatment treatment (medication + behavior therapy)
Why Non-Stimulant Treatments For ADHD? Problems with the stimulants • Scheduled II drugs (abuse liability, diversion, medico-legal concerns) • 30% - 40% do not adequately respond or cannot tolerate stimulant treatment • Side effect profile adversely impacting sleep, appetite, mood and anxiety • Concerns about growth suppression and tic development
ADHDMotor Vehicle Driving • Study of 16 to 22 year olds • 35 with ADHD (not on medication) • 36 controls • Significantly more drivers with ADHD • drove without a license • had licenses revoked or suspended • had multiple crashes (2+) • had multiple traffic citations (3+), especially for speeding Subgroups of ADHD with comorbid oppositional defiant or conduct disorder were at highest risk Barkley et al. Pediatrics 1993;92:212.
ADHD:Impairment in ADHD Psychiatric comorbidity School failure Poor peer relationships Legal difficulties Smoking and substance abuse Accidents and injuries Family conflict Parent stress
ADHD Etiology and Impact Summary • ADHD is a neurobehavioral disorder with a • complex etiology • neurobiologic basis • strong genetic component • ADHD • affects millions of people of both genders • persists through adolescence and adulthood in a high percentage of cases • can have negative impact on multiple areas of functioning • Although stimulants are highly effective in the treatment of ADHD, 30%-40% of patients do not improve of or cannot tolerate them
Clinical Pharmacology and Efficacy Lesley Russell, MRCP Senior VP, Clinical Research Cephalon, Inc.
Pediatric ADHD Development Program sNDA Phase 2 Phase 3 Phase 3B Phase 1 Study 113 (BA) n=24 Study 206 (PK/DR) n=20 Study 309 (DB,PC) n=198 Study 3044 (OL) n=303 Study 207 (DR) n=47 Study 310 (DB,PC) n=189 Study 213 (POP) n=248 Study 311 (DB,PC) n=246 Study 312 (OL, EXT) n=533
Modafinil Pharmacokinetics:Children/Adolescents • Dose proportional over the studied dose range • Absorption • Tmax 2-3 hours – 1 hr delay with food • Distribution • V/F increases linearly with weight • Metabolism • Primarily by liver (<10% excreted unchanged in urine) • Two primary metabolites; modafinil acid and modafinil sulfone • Higher levels of modafinil sulfone in younger children • Elimination • Time and age dependent • Clearance changes over time • steady-state reached by week 6 • Decrease in clearance gradual with pronounced shift between 9 to 11 years • t½ 7 hours in younger children; t½ 15 hours in adults
Phase 2 ADHD (Study 207) ADHD Rating Scale (Home Version) • Double-blind, randomized, four period, crossover study (N=48)
200 AUC μg • hr/mL 150 146 130 118 100 >30 kg, 300 mg <30 kg, 300 mg >30 kg, 200+200 mg Weight and Dose Groups Identification of Target Systemic Exposure
PK/PD Modeling • Estimated systemic exposure associated with PD response • 150 μg•hr/mL • Estimated doses • 340 mg <30 kg • 425 mg ≥ 30 kg
Systemic Exposure Following Administration of modafinil up to 21 Weeks (Phase 3 Studies) 350 300 250 N=177 N=42 AUC μg • hr/mL 200 153.5 149.9 150 100 50 340 mg 425 mg Dose Includes patients receiving 340 mg (< 30 kg) and patients receiving 425 mg (≥ 30 kg)

![Tell a Story! [Be the Batman]](https://cdn4.slideserve.com/7369331/slide1-dt.jpg)