Download

1 / 29
300 likes | 536 Views
Augmentation of the antidepressant action of sertraline with triiodothyronine (T3): Clinical efficacy, adverse effects and predictors of response. Dept of Psychiatry. 14 th Annual Israeli Society of Biological Psychiatry, Kibbutz Hagoshrim 2010 תחרות מדעי יסוד. Aviva Cohen.

E N D
Augmentation of the antidepressant action of sertraline with triiodothyronine (T3): Clinical efficacy, adverse effects and predictors of response Dept of Psychiatry 14th Annual Israeli Society of Biological Psychiatry, Kibbutz Hagoshrim 2010 תחרות מדעי יסוד Aviva Cohen
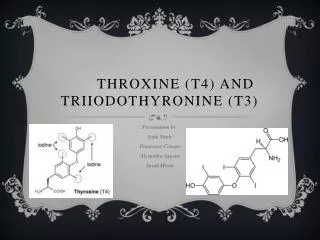
T4 (Thyroxine) T3 (3,5,3’ Triiodothyronine)
Depression Hypothyroidism 5-10% Thyroid disorders found Increased prevalence of depression Depression and the Thyroid Gland
Depression and the Thyroid Gland • Thyroid dysfunction may be associated with diminished response to antidepressant treatment • Supplementation of antidepressant treatment with thyroid hormones (T3 and T4) reported to enhance response in refractory patients and to accelerate onset of antidepressant effect
Augmentation of Tricyclic Antidepressants by T3: Meta-analysis • 8 studies, 292 patients • Non-psychotic depression refractory to TCAs • Patients euthyroid • 25-50 µgT3 • 2 times greater response rate in patients treated with T3, corresponding to 23.2% absolute improvement in response rates compared to placebo Aronson et al, Arch Gen Psychiatry. 1996; 53:842-8.
The use of liothyronine (T3) in Major Depression treated with SSRIs • 3 small augmentation studies (N=12-25) all showed response rates of 35%-42% to the addition of T3 after non-response to 6-8 weeks of SSRI • T3 as good as Li and better tolerated as augmentation after failure of 2 AD • Enhancement studies find inconclusive (Posternak) or conflicting (Appelhof vs Cooper-Kazaz) results • T3 well tolerated in most studies • Association of response to T3 with thyroid function needs more studies
F(Treatment) 5.68; df = 1, 98; p=.02 HRSD Scores - Intent to Treat ANCOVA 38% vs 58% Pearson Chi2 5.14, df=1, p=.02, OR=2.69, CI=1.16-6.49
0.5 0.25 0 -0.25 Change in TSH (IU/L) Over the Treatment Course (Post - Pre) -0.5 -0.75 -1 -1.25 Non-Remitter Remitter -1.5 -1.75 SERT-T3 Change in TSH and Remission T3 Baseline Levels and Remission x2 = 5.08, df = 1, p = 0.02 x2= 5.63, df = 1, p< 0.02
Objectives of the Study • To evaluate efficacy, adverse effects appropriate timing of T3 as a supplement to the treatment of MDD with the SSRI, sertraline • To determine the relationship to thyroid function of (T3) and anti-depressant treatment
Study Design • Open Label • Major Depression, non-psychotic • Participating center - Hadassah – Hebrew University Medical Center, Jerusalem Israel
Study Design – Inclusion Criteria 1) Diagnosis of Major Depressive Episode (MDE) in the context of Major Depressive Disorder (UPD), according to DSM-IV criteria, without psychotic features. 2) Hamilton Depression Scale (HRSD) total ≥16 with item 1 (depressed mood) >2. 3) Age 18-70 years. 4) Male or female 5) Competent and willing to give written informed consent.
Study Design – Exclusion Criteria 1) Clinical hyper- or hypothyroidism or other thyroid illness (including sub-clinical hypothyroidism) 2) Neurological or other physical illness that may impact upon the study or limit prescription of the study medications 3) Lifetime history of substance or alcohol dependence or of abuse in the preceding 12 months Significant suicidal risk (HRSD item 3 [suicide] >2) Pregnant or lactating women
Study Design – Exclusion Criteria 6) Treatment with the antidepressant, sertraline in current episode 7) Current episode more than 2 years 8) More than one anti-depressant trial during the current episode and/or augmentation strategy 9) Co-morbidity with any psychotic disorder, mania, PTSD, eating disorder
Interventions and Major Outcomes • Patients were treated with sertraline 50 mg\day for 1 week and 100 mg\day thereafter if tolerated for 4 weeks • Patients who fulfilled the criterion for remission according to HRSD <7 continued treatment with sertraline alone • Patients who did not fulfill the criterion for remission received supplementary treatment with T3, 20 mcg\day for the first week and 40 mcg\day thereafter if tolerated
Patient enrolment 27 50 mg/d sertraline (SERT) - first week 100 mg/d thereafter 1 drop out at week 0, lost to follow up, not included in study 26 week 0 26 Included in study 2 drop outs week 2; side effects 19 non-remitters 24 continued SERT 100mg 24 Week 4 17 non-remitters Add T3 20 mcg/d –1week 40 mcg/d - thereafter 5 remitterscontinue SERT alone 2 drop outs week 4 1-overseas 1-psychotic features 22 Week 8 7 SERT-T3 remitters 1 SERT -alone non-remitter 4 SERT alone remitters 1 drop out week 8, side effects and lack of response Non remitter, LOCF 10 SERT-T3 non-remitters 1 drop out week 10, lost to follow up, but remitted LOCF 1 drop out week 10, lost to folow up, but remitted, LOCF 7 SERT-T3non-remitters Discontinue T3 (2 wk) 3 SERT -T3 remitters Continue T3 (2 months) 1SERT-T3non-remitters Discontinue T3 (2 wk) 6 SERT-T3 remitters Continue T3( 2 months) 5 SERT alone remitters 19Week 12 8 SERT-T3 Non-remitters 14 remitters 9 SERT-T3 & 5 SERT alone
Remission Rate of Patients Augmented with T3 after 4 Weeks of sertraline Treatment
Conclusions • Efficacy in adding T3 as augmentation at 4 weeks • Tolerable side effects • There was a change in thyroid function tests due to T3 treatment, but no correlation was found with remission
Where to? • Larger sample, recruitment • Double blind • Variable doses of sertraline • Variable times of augmentation • Other SSRIs • Further testing of thyroid function including genetics • Longer duration 15 weeks
Acknowledgements Thank you Prof Bernard Lerer, Dr. Rena Cooper-Kazaz (Supervisors) Prof Benjamin Glaser (Endocrinology Adviser)(Hadassah – Hebrew University Medical Center)