Download
1 / 24
240 likes | 382 Views
Volumetric Airflow Gauge. Guy Guimond, UPMC Center for Emergency Medicine Eric Reiss, Systems Manager, Swanson Institute Matthew Chakan Michael Nilo Justin Kiswardy. April 10, 2007. University of Pittsburgh, Department of Bioengineering. Background & Significance.

E N D
Volumetric Airflow Gauge Guy Guimond, UPMC Center for Emergency Medicine Eric Reiss, Systems Manager, Swanson Institute Matthew Chakan Michael Nilo Justin Kiswardy April 10, 2007 University of Pittsburgh, Department of Bioengineering
Background & Significance • Estimates of over 500k 911 calls daily, 35% involve cardio-pulmonary failure1 • Most common means of initiating breathing in-field is use of mechanical ventilator (BVM) • BVM systems used in patient transport w/in hospital or when true mechanical ventilators not accessible 4
Background & Significance • Most Healthcare Providers trained to “inflate based on resistance” w/ recommended introduced air @ 400-600ml/cycle for average adult patient2 • As result of HP making on-site estimates, dangerous air flow rates & pressures administered to patients have been observed • Documented side-effects: lung tissue damage, lung compliance, gastric distension, regurgitation • Clinical Study showed ~40% patients experienced gastric distension & 65% morbidity3 5
Project Objectives • Design a universal gauge capable of measuring airflow volumes that is easy to learn, operate, and comprehend for the user • Device must be lightweight, portable, and adaptable to most standard ventilators/BVM’s (Laerdal, Ambu, First Responder) • Features adaptable for incorporation into a learning environment (EMT classes)
Design Alternatives • Disposable vs. reusable • many BVM systems are intended for one-time use (pp. ~$20-50) • disposable systems come w/ disposable attachments (PEEP gauge, pH indicator, etc.) • reusable systems are able to be flashed via autoclave • market allows much higher cost (pp. ~$100-400) • How will the airflow volume be measured • pinwheel mechanism using highly compliant metal pin • no external power source, sterilizable, inexpensive manufacturing/ price-point, low-level accuracy, malfunction issues, rotary gauge may be difficult for user to read • electrical circuit similar to mass flow device, incorporating microcontroller, thermistors to measure airflow volume • high-level of reproducible accuracy, requires external power source, computerized manufacturing, no autoclave, higher cost Decision: VAG is intended to be reused and may be sanitized w/ EtOH. Reusable device allows for higher production costs creating broader market. Decision: electrical circuit minimizing error range & malfunction issues while maximizing ease of manufacturing
Basic Component Selection • Air flow sensor requirements: • Flow range > 1.6 L/s • Size < 38 in3 • Cleanable with medical products (e.g. Isopropanol) • Display requirements: • Two decimal place precision → 3-digit • Digit height > ¼” • Microcontroller requirements: • Relatively large RAM and ROM • Enough pins to operate sensors and displays
Component Integration • Electrical needs of basic components were identified and ordered • 9V → 5V → 2.2V • Bridging components were selected • Voltage Regulator (9V → 5V) • Resistors (5V → 2.2V) • Component compatibility was checked by verifying complementary electrical characteristics (AIout < BIin)
Extra Feature Addition • The air volume will change after reaching the patient’s lungs • Charles’ Law: V2 = V1 * (T2/T1) • A thermistor was added to measure ambient temperature • The rate of artificial respiration is important • A Flashing LED metronome was added to indicate the rescue breathing rate • The user needs to know when to replace the batteries • Independent battery sampling and alert systems were added
CircuitOperation • A C program was written for the microcontroller to: • Measure: • Instantaneous air flow rate • Ambient temperature • Battery voltages • Display: • Cyclic air volume sum • Rescue breathing metronome • Low battery voltages • Hold maximum cyclic air volume sum for easier user reading • Reset air volume sum to zero for next cycle
Product Engineering Objectives • Build a casing that • Prevents water from contacting the electrical circuit • Diminishes mechanical damage to the circuit • Seals the circuit and all small parts from the airflow path • Houses two 9V batteries • Fits the standard fittings of both the bag and valve attachments • distal tubing 15mm • proximal tubing 23mm • Weighs less than 100g without batteries • Is not cost prohibitive
Prototype Development • Initial prototypes made of wax • Current SLA prototype • Finished product
Project Management Dec. | Jan. | Feb. | Mar. | Apr. Project Introduction Conceptual Design Electrical Design Circuit Program Mechanical Design Casing Development V and V Written Deliverables Responsibilites: Matt Chakan: Circuit Design and Fabrication, Microcontroller C Program Michael Nilo: Mechanical Design and Fabrication using SolidWorks Justin Kiswardy: Verification and Validation, Written Deliverables
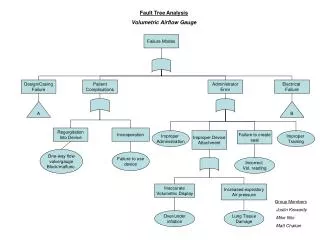
Quality Control Considerations • Class I medical device • ISO 13485 rule 7.1 & 7.2 “non-invasive devices intended to act as calibrator, monitor, or tester while connected to an active type II, III device…..is class I” • VAG must comply with FDA’s Code of Federal Regulations 21.CFR.868.9 “ventilator tubing is device intended for use as conduit for channeling of gases between ventilator and patient during ventilation of patient…device is exempt from pre-market notification procedures” Result: As class I device subject only to general controls. Must register device with the FDA and comply with good manufacturing techniques providing reasonable assurance of safety and effectiveness of product. • Risk Analysis • Initial hazard analysis * identified two potentially catastrophic risks: components of device break and enter patients airway and device malfunctions and blocks tubing. * risks minimized by requiring that the user place device above the one-way valve, small components will not have direct access to inside tubing (casing), ease of incorporation and removal from BVM • Failure Modes/Effects analysis
Verification & Validation • Optimize power source • one vs. two 9V batteries: conduct tests to determine difference in battery life • one 9V=~15 min., two 9V=+2 hrs. • analyze outcome vs. increased cost/inconvenience to user • Accuracy tests for display • clinical studies show over-inflation by only 100ml can cause gastric distension • desired accuracy range +/- 50ml air • laerdal manikin w/ built in volume gauge • Survey administered to various doctors, nurses, and other Healthcare Providers involved in the treatment/use with BVM systems. • Outcome of survey should allow the fine-tuning of the VAG (ie., the elimination or addition of features) and will be easier to understand specific market needs
Features & Benefits • Potential disadvantages • periodic battery replacement/testing (increases maintenance tasks required of user) • non-sterilizable (limit market size) • does not account for air escaping face/mask seal • Summary of features • a cost-effective volumetric airflow gauge that can be incorporated into any standard BVM system • provides numeric display of air volume introduced to patient during in-field/hospital rescue • provides high level of accuracy (w/in +/-50ml) • may be disinfected for repetitive use • eliminates comorbidity associated w/ over/under inflation (gastric distension, lung damage, regurgitation), reduces hospital stay/costs • built in LED metronome may be used for training purposes/user awareness 6
Market Potential • Market size & pricing • 2005 sales: Zoll med. ~$248 mil., Ambu ~$116 (respiratory care) • more than $1.3 billion spent (US) on ventilators, oxygen therapy systems, and airway management devices in 2004 • reusable PEEP valves $100-200, disposable pH indicators $50-100 • Current competition • mechanical transport ventilators: manually set the desired flow rate, pulsatile flow based on PIP and PEEP, bulky (20-40 lbs.), expensive (>$1500) • hand-held monitors: battery operated, lightweight, complicated setup, expensive (+$400) • Future competition? • r&d geared towards design of eff. volume gauge 8 9 7 10
Moving Forward • Finish testing and validation • make necessary adjustments according to results of survey • testing through UPMC Center for Emergency Medicine • Design packaging and instruction/troubleshooting manual • Submit SBIR phase I proposal
Acknowledgements • Mr. Guy Guimond & UPMC Center for Emergency Medicine • Dr. Hal Wrigley and Dr. Linda Baker for providing funding • Department of Bioengineering, University of Pittsburgh Thank You Department of Bioengineering University of Pittsburgh
Overview • Incorporation of volumetric airflow gauge into a standard mechanical ventilator/bag-valve-mask system (BVM) • Intended to provide user w/ volume of air introduced to patient with each squeeze of the bag • Intended users include: EMT specialists, trained nursing staff, doctors and other healthcare providers
Citations Citations 1. Davidoff F, DeAngelis CD, Drazen JM, Hoey J, Hojgaard L, Horton R (2006). Emergency Cardiac Care. Prehospital Emergency Care; Vol. 10; 36-48. 2. Kuhns R., Davis J. (2004). A work measurement evaluation of emergency medical services. IIE Annual Conference and Exhibition 2004; 3431-3467. 3. American Heart Association (2005). AHA guidelines for CPR and ECC. Vol. 112; Issue 4; 14-20; 126-131. 4. Von Goedecke A, Wagner-Berger H, Stadlbauer K, Krismer A, Jakubasko C, Bratschke C, Wnzel V, Keller C. (2004). Effects of decreasing peak flow rate on stomach inflation during bag-valve-mask ventilation.Resuscitation; 63: 131–136. 5. International Liaison Committee on Resuscitation. 2005 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations.Circulation. 2005; 112: III-1–III-136. 6. Nolan J. (2001). Prehospital and resuscitative airway care: should the gold standard be reassessed? Current Opinion in Critical Care; 7: 413–421. 7. Wenzel V, Keller C, Ahamed H, Volker D, Lindner K, Brimacombe J (1999). Effects on smaller tidal Volumes during basic life support ventilation in patients with respiratory arrest: good ventilation, less risk?Resuscitation; 43: 25–29. • Sheperd C.,(2006). Reflection on a patient's airway management during a ward-based resuscitation. Nursing in Critical Care; Vol. 11, 217-2 23 • Life Medical Supplier, www.lifemedical.com • Miraclemed, www.miraclemed.com, Seattle, WA.