Download
1 / 21
240 likes | 635 Views
The SAD Story of Aortic Stenosis. Death by Exercise Doug Pereira. How the heart functions normally. Blood is received into the right atrium from the superior vena cava The right atrium pumps blood into the right ventricle, through the tricuspid valve

E N D
The SAD Story of Aortic Stenosis Death by Exercise Doug Pereira
How the heart functions normally • Blood is received into the right atrium from the superior vena cava • The right atrium pumps blood into the right ventricle, through the tricuspid valve • The right ventricle pumps blood through the pulmonic valve into the pulmonary arteries • The blood exchange gas with the air in the alveoli, and flows into the pulmonary veins • The left atrium receives blood from the pulmonary veins • The left atria pumps blood into the left ventricle via the mitral valve • The left ventricle pumps blood into the aorta, via the aortic valve
What if this doesn’t work correctly? • Normally, the output of the right and left sides of the heart are equal. • If the myocardium doesn’t contract well, a valve is stuck/leaky, vessels are obstructed, or an arrhythmia throws the timing of contractions out of sync, the output of one side will decrease. • This causes blood to pool in the veins, in the pulmonary veins if the left side is deficient, or in the systemic veins if the right side is deficient
What symptoms does this cause? • Dyspnea, due to pressure in the pulmonary vessels increasing (if the left side is failing) or decreasing (if the right side is failing), preventing proper blood flow and gas exchange, especially during exercise or while lying down • Fatigue due to decreased systemic perfusion • Angina due to decreased coronary perfusion • Tachycardia due to increased heart rate in an attempt by your body to raise cardiac output • Other symptoms, such as renal failure due to decreased systemic perfusion, or liver failure due to blood pooling in the portal vein
How this diagnosed? • A thorough history and physical exam, with special attention to heart sounds and pulse quality • Measurement of B-type naturietic peptide, a protein secreted by the ventricles in response to pressure or volume overload • An EKG to determine if any arrhythmias are present, which may have caused or contributed to the heart failure • An echocardiogram, to evaluate how the myocardium is contracting, whether any valves are stuck/leaky, and measurement of pressures and volumes • Other tests (nuclear scan, cardiac CT/MRI, cardiac catheterization, etc.) if needed, based on the findings from the above
An example of how this can happen • If the aortic valve becomes stuck (due to calcification or scarring), the left ventricle has to generate much greater pressures to open the valve in order to eject blood into the aorta • Since the left ventricle has to work harder, it will get thicker in order to generate greater pressures. • But this comes at a huge cost…
First, a few terms defined • Cardiac output is defined as stroke volume (the amount of blood ejected in one beat) times heart rate • Stroke volume is defined as end-diastolic volume (total volume of blood at the end of diastole) minus end-systolic volume (remaining blood in the ventricle after systole) • Afterload is the amount of pressure the left ventricle needs to generate in order to eject the stroke volume into the aorta • Preload is another name for end-diastolic volume • Inotropy is the strength of the heart’s contractions
Or, if this confuses you • Think of a water pump. • The amount of water in the reservoir is preload • The strength of the water pump is inotropy • The size of the nozzle is afterload • To get an equivalent volume of water through a smaller nozzle vs a larger one, in an equivalent time span, requires greater pressure
Back to the story • Since the left ventricle has become thicker due to effects of the increased afterload caused by the stuck aortic valve, end-diastolic volume is reduced, leading to decreased stroke volume • In an attempt to raise cardiac output, tachycardia results • This leads to less time available for the left ventricle to fill with blood from the left atrium, decreasing end-diastolic volume even more, leading to vicious cycle
Aortic stenosis is a SAD story • Syncope (fainting) results during exercise. This is due to the arteries in your muscles dilating to allow increased perfusion. Normally, your cardiac output will rise to maintain blood pressure. However, aortic stenosis causes cardiac output to be essentially fixed, leading to a drop in blood pressure, which leads to decreased brain perfusion • Angina results due to the decreased end-diastolic volume causing decreased coronary perfusion, which leads to myocardial ischemia • Dyspnea results from excess blood remaining in the left atrium, increasing pulmonary venous pressure
What happens if left undiagnosed? • Eventually, pressure and volume in your left atrium will become so large that it enlarges, putting pressure on the SA node, which over-stimulates it. This leads to atrial fibrillation (the atria are quivering instead of contracting). This drops preload by 30%, and can lead to strokes due to stagnant blood clotting. It’s also very unpleasant. • Likewise, pulmonary venous hypertension will lead to pulmonary arterial hypertension, which strains the right ventricle. Unlike the left ventricle, the right ventricle is a pussy, and will fail at the slightest pressure overload. This leads to liver failure due to blood pooling in the portal vein, and lower extremity edema due to blood pooling in their veins. • This decreases preload, decreasing stroke volume even more. • Eventually, the left ventricle can no longer cope with the afterload, and it will dilate and fail. • 50% mortality in 3 years.
How is it diagnosed? • A history of syncope, angina, and dyspnea on exertion • A weak, late pulse • A blood pressure reading where the systolic pressure is very close to the diastolic pressure, reflecting decreased stroke volume • A harsh systolic murmur that increases in intensity when the patient squeezes their hand tightly (which increases afterload)
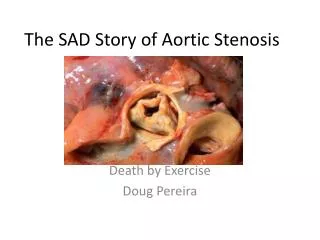
Explanation of the picture • The aortic valve is heavily calcified, hence it being bright white • The left ventricle walls (labeled ‘S’ for septum and LVPW for “left ventricular posterior wall”) is severely thickened due to pressure overload, and it’s volume is reduced • The left atrium is very enlarged due to backflow from the ventricle
Why do an echcardiogram? • It can quantify severity and determine how best to treat • It can tell you something very important: the pressure gradient across the valve, which has huge implications in deciding whether or not to do aortic valve replacement surgery (the only definitive cure)
The transaortic pressure gradient • Determined by measuring the pressure across the valve. • A normal valve has no gradient • *Usually* in AS, this will be high, and will increase with stress (exercise or dobutamine). This is important in the next slide. • Can be used to calculate the area of the valve, in square centimeters, by dividing cardiac output in liters/minute by the square root of the gradient in mmHg • So if someone has a cardiac output of 5.4 L/min and a transaortic gradient of 81 mmHg, the aortic valve area will be 0.6 cm^2. This is severe AS, as it’s less than 0.8 cm^2 (and normal valve area is 3.0-4.0 cm^2)
But what if the gradient is low and doesn’t increase with stress? • If the gradient is low, and does not increase much with stress (dobutamine or exercise), the left ventricle has already failed. This is called “low inotropic reserve” • Aortic valve replacement surgery will not provide much benefit, as the reason for the valve being narrow is due to the left ventricle not being strong enough to open it. • It will also be extremely risky, as cardiac surgery imposes a lot of stress on the heart, and they may not be able to be weaned off the heart-lung machine • Nevertheless, the cardiologist should ask for a cardiac surgeon’s opinion on performing aortic valve replacement, as it’s better than medical therapy alone, by decreasing afterload and thus the heart’s strain.
How do we treat patients with AS? • Percutaneous balloon aortic valvotomy: placing a balloon in the aortic valve to dilate it. This relieves symptoms, but only for a few months. Your patient is not a German luxury car, and we can’t keep taking them to “the shop” every few months for a “tune up”. Generally, it’s only used when they have to go for urgent non-cardiac surgery • Traditional aortic valve replacement surgery: The patient is placed on a heart-lung machine, the aorta is opened, the valve is excised, and a mechanical or cadaver valve is sown in. A cadaver valve wears out an has to be replaced every decade or so, but a mechanical one requires lifelong anticoagulation to prevent clots from forming. Cadaver valves are generally used for the old, and mechanical ones are used for the young • Percutaneous aortic valve replacement: A cadaver valve inside a stent that’s collapsed onto a catheter, which is threaded up the femoral artery, through the aorta, and into the side of the old valve. It’s then expanded, and pushes the old valve leaflet out of the way. A good option for those with low-to-no inotropic reserve
But what of the patients who wouldn’t benefit from aortic valve replacement, or who are waiting for it? • Medication, usually digoxin to improve filling and control any atrial fibrillation, ranolazine for angina, and beta blockers to decrease the heart’s strain • The ImCardia by CorAssist is a spring device that can transfer the force generated during systole to open the valve into a force that can hold the ventricle open during diastole, greatly improving filling • A left ventricular assist device is a surgically-placed pump that can rest the heart by taking over it’s work, and hopefully allow it to recover enough strength so aortic valve replacement surgery can be done, or as a final therapy • Avoidance of streneous activity (yard work, sex, etc.), and avoidance of drugs that cause vasodilation