Download
1 / 21
260 likes | 655 Views
WOC Nursing and Pressure Ulcer Prevention. History and Current Status Heath Brown RN, WOCN Wellstar Kennestone. History. 1958: Dr. Turnbull created role of “ET” (Enterostomal Therapist) Purpose: Provide rehabilitative care to new ostomy patients

E N D
WOC Nursing and Pressure Ulcer Prevention History and Current Status Heath Brown RN, WOCN Wellstar Kennestone
History • 1958: Dr. Turnbull created role of “ET” (Enterostomal Therapist) • Purpose: Provide rehabilitative care to new ostomy patients • First ETs: individuals who had an ostomy or a family member with an ostomy
Milestones in Role Development • 1960s: Formal training programs developed • 1976: RN established as “entry into practice” • 1983: Baccalaureate degree required for entry into practice • Scope of practice expanded to include wound care and continence care
WOC Nursing in 2011: Statistics • Approximately 5000 WOC nurses in US • 60–70% prepared at baccalaureate level – 30 – 40% at master’s level or higher • Practice settings: acute care (majority); HH; outpatient
Certification in WOC Nursing • Pathways: • Completion WOCN-accredited program (10 weeks full time: theory + clinical) • Experiential pathway: 1500 practice hours + 50 CE hours for each area for which certifying
WOC Nurse Role in 2011 • Wound Care primary focus for most WOC nurses • Diabetic foot care • Fistula management • Consultation/mgmt regarding wound mgmt • Pressure ulcer prevention (agency wide programs)
WOC Nurse Role in 2011 • Ostomy Care • Preop counseling/ stoma site marking • Postop: pouch selec- tion/instruction in self care • Rehabilitative care and counseling (sexual counseling)
WOC Nurse Role in 2011 • Continence Care (Setting Dependent) • Acute Care • Staff education re: CAUTI prevention • Staff education re: correct use indwelling bowel dng systems • Skin care and containment
Changes and Challenges • Increasing focus on role of consultant vs role of caregiver/educator • Increasing responsibility for development agency-wide programs for pressure ulcer prevention and evidence-based WOC care • Increasingly complex wound and fistula care (e.g., negative pressure wound therapy) and more challenging stomas • Advanced Practice WOC Nurses increasingly common in outpatient care
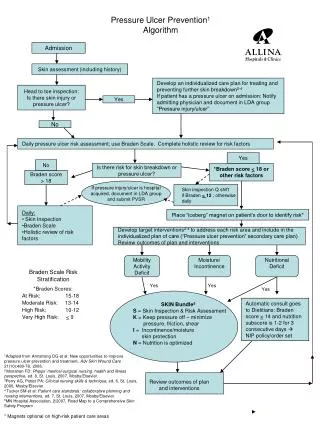
Pressure Ulcer Prevention • Most PUP Programs are essentially the same: Catch ‘em at the front door (Assessment) Prevent ‘em while they’re here (Prevention)
Components of aPUP Program * Initial skin assessment on admit * Daily Risk Assessment for all patients * Reassess skin daily or more often * Manage moisture – keep dry and moisturize skin * Optimize nutrition & hydration * Minimize pressure
1 Initial Skin Assessments • Every Admitted Patient • Required by CMS to show what was POA • Good Nursing Practice
Braden Scale • Sensory perception • Moisture • Activity • Nutrition • Mobility • Friction/shear
2 Risk Assessment for PUs • Daily or more often for all patients • Different scores should reflect different preventive strategies
3. Reassess Skin Daily • Q Day or Q Shift
4 Prevention: Manage Moisture • Keep the patient dry • Moisturize the skin
5 Optimize Nutrition & Hydration • Attend to the microclimate of the skin – calories, hydration, protein • Registered Dietician Consults
6 Minimize Pressure • Turn Every 2 hours or more often based on clinical condition • Use Pillows to redistribute weight • Offload heels • Use Pressure redistribution Surfaces to maximize the time/pressure ratio
On a Programmatic Level Monitor, Monitor, Monitor Continuously Re-evaluate your processes
Monitoring our programs by conducting quarterly prevalence surveys • Monitoring and conducting RCAs of HAPUs • Participating in almost every aspect of nursing with an eye towards protecting patients skin from pressure and reevaluating processes • Device related pressure ulcers