Download
1 / 47
470 likes | 611 Views
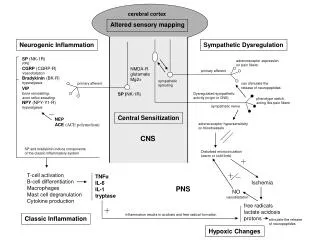
The CNS Role and Outcomes Management. Evelyn Taverna, RN, MS, CCRN, CNS Guest Lecturer: N 226 February 19, 2003. Overview . Purpose: to extend the traditional role of case management to patient population based clinical resource management

E N D
The CNS Role and Outcomes Management Evelyn Taverna, RN, MS, CCRN, CNS Guest Lecturer: N 226 February 19, 2003 California Pacific Medical Center
Overview • Purpose: to extend the traditional role of case management to patient population based clinical resource management • Develop systems to manage patients across the continuum - from inpatient to extended care to home health • Create teams to effectively manage and integrate departmental activities in a cost effective, outcome driven manner California Pacific Medical Center
Population Based Teams • Cardiology • Cardiovascular Surgery • Medicine • Neurology/Neurosurgery • Obstetrics • Oncology • Pediatrics • Pulmonary • Surgery/Orthopedics California Pacific Medical Center
Team Members • Clinical Nurse Specialists • RN Case Managers • Social Workers • Administrative Assistants • Data Analysts • Quality Coordinators • Physician Champions California Pacific Medical Center
CPMC Quality & Clinical Resource Management Model CLINICAL MANAGEMENT RESOURCE MANAGEMENT Clinical Nurse Specialist Population Based Case Manager Social Worker Patient/Family Based Administrative Assistant Support QUALITY MANAGEMENT OUTCOMES MANAGEMENT STAFF MANAGEMENT DEPARTMENTS UR PHYSICIANS HOSPITALISTS DISCHARGE PLANNING SOCIAL SERVICES UTILIZATION MANAGEMENT California Pacific Medical Center
Quality & Clinical Resource Management Model CLINICAL NURSE SPECIALISTS Cardiology, Cardiac Surgery, Interventional Endoscopy, Medicine, Neonatal, Neurology/Neurosurgery, Oncology, Pediatrics, Perinatal, Pulmonary, Surgery/Ortho Quality Improvement Focus • Clinical Management • Protocols • Best practice guidelines • Clinical consultation • Staff education • Complex case review • Resource Management • Benchmarking • MD comparisons • LOS/level of care • Cost/resource analysis • Resource utilization • Outcomes Management • Quality, cost, service • Data analysis/research • Clinical effectiveness • PI projects • Sutter initiatives California Pacific Medical Center
The CNS as Team Leader • Masters prepared expert nurse clinician • Manage clinical resources • Define care requirements (best practices) • Monitor their impact on outcome achievement • 60% of time actively involved with patients • Daily interaction with patients, families, clinical staff, nurses, and physicians • Continually evaluate patient care needs • Individuals and aggregate population • Seek opportunities for improvement California Pacific Medical Center
Project Selection • External Sources/Needs • Mandatory – JCHAO Core Measures & Standards • State Requirements - OSHPD • Sutter Initiatives • Press-Ganey Patient Satisfaction Survey • VHA Programs • Internal Sources California Pacific Medical Center
Project Selection External Regulatory Requirements JCAHO CORE Measures - 2002 • CHF • Perinatal Outcomes JCAHO CORE Measures – 2003 • Community Acquired Pneumonia California Pacific Medical Center
Project Selection JCAHO Standards • Pain Management – Jackie Phan, CNS • Patient Safety- Gail Guthrie, CNS & Phyllis Erickson, CNS • Medication Error Reduction – Evelyn Taverna, CNS California Pacific Medical Center
Project Selection External Requirements • California CABG Outcomes Reporting Program (CCORP) – Jill Ley, CNS • Crusade Study & National Registry for Myocardial Infarction (NRMI) – Evelyn Taverna, CNS • ACOS Accreditation – Alice Mack, CNS • National Practice Recommendations: • AHA, AHCPR, etc. California Pacific Medical Center
Developing Clinical Questions • Institutional Sources • Quality committees • Performance Improvement teams • Product lines • Clinician Sources • Clinical observations • New products/techniques • Evidence-based practices California Pacific Medical Center
Current Projects • Medication Error Reduction • Coumadin dosing project • Range-dosing protocol • Patient controlled analgesia protocol • New Procedures • Bariatric surgery outcomes • Continuous renal replacement therapy • Off-pump CABG outcomes • Outcomes Management • Interventional endoscopy database • Plavix research and practice change • VBAC – Best practice California Pacific Medical Center
Current Projects • Medication Error Reduction • Coumadin dosing project • Range-dosing protocol • Patient controlled analgesia protocol • New Procedures • Bariatric surgery outcomes • Continuous renal replacement therapy • Off-pump CABG outcomes • Outcomes Management • Interventional endoscopy database • Plavix research and practice change • VBAC – Best practice California Pacific Medical Center
Agency for Health Care Policy & Research(AHCPR) AHA,ACC VHA CMRI HBSI Fathom Midas NRMI 4 Crusade Benchmarking Resources California Pacific Medical Center
Influencing Physician Practice • The CNS is the “point person” for providing cost, service, and quality information to the Medical Staff to guide data drivenpractice changes which: • reduce cost variations • decrease overall cost • maintain quality outcomes • improve service California Pacific Medical Center
Cardiology CNS • Acute Coronary Syndrome • CHF • Pacemaker Study • Atrial Fibrillation • Complex patients • clinical • education • discharge planning California Pacific Medical Center
Cardiology: • AMI • ED chest pain protocol • STEMI and NSTEMI protocol • Crusade & NRMI 4 data – Focus on NSTEMI outcomes • IIb/IIIa inhibitor use and bleeding • interventional procedures • Sutter Cardiovascular Services Initiative • AMI task force • CHF committee • CHF • ACE inhibitor use and discharge instruction outcomes & readmission California Pacific Medical Center
AMI Outcome Measures • Aspirin at arrival • Beta blocker at arrival • Median time to thrombolytic therapy • Median time to PTCA • Aspirin prescribed at discharge California Pacific Medical Center
AMI (cont.) • Beta blocker prescribed at discharge • ACE I at discharge for LVSD • Adult smoking cessation advice • Inpatient mortality • Lipid-lowering agent at D/C California Pacific Medical Center
AMI Strategies • ED Chest Pain Risk Assessment • Acute Coronary Syndrome Protocols/Order Sets • AMI Standard of Care • AMI Guide to Recovery California Pacific Medical Center
AMI Case Study Mr. M is a 54 year old man admitted with c/o of chest pain which began while watching the 49’ers playoff game. Patient lives with wife and works in law enforcement. Symptoms included: • Constant, substernal chest pressure (5/10) • Diaphoresis California Pacific Medical Center
AMI Case Study PMH: • CAD, S/P angioplasty in 1989 • Diabetes • Hypertension • Hypercholesterolemia • Current smoker Medications: • Atenolol and Glucophage • Allergic to Aspirin and Motrin California Pacific Medical Center
AMI Case Study Physical Exam: • Vital stable with bradycardia of 58 • Oxygen sat 96% on 2 liters • Lungs clear, no JVD Labs: • Elevated cardiac markers • Glucose – 295 EKG: • ST elevation in inferior leads California Pacific Medical Center
AMI case study Interventions: • Plavix • Nitro • Morphine • Heparin • Primary PTCA with GP IIb/IIIa inhibitor during/after PTCA • Door to balloon time = 100 min. California Pacific Medical Center
AMI case study Discharge planning Cardiac rehab (PT, OT, Dietary) Smoking cessation advice Stress management Aspirin, Plavix, Beta blocker, ACE I inhibitor, statin California Pacific Medical Center
ACUTE MI DEMOGRAPHICS AND RISK FACTORS California Pacific Medical Center
AMI Opportunities for Improvement • Emergency Department: • Door to EKG time • Chest pain Risk Assessment Protocol • CPK & Troponin utilization • Cath Lab: • Door to Balloon time • Critical Care & Telemetry • Analysis of bleeding requiring intervention • Patient Education material • Cardiac Rehab California Pacific Medical Center
CARDIOLOGY SEVICE LINE 2001 – 2002 California Pacific Medical Center
CARDIOLOGY SERVICE LINE COST DATA 2001 – 2002 California Pacific Medical Center
Congestive Heart Failure System-wide PI Project High volume, high resource utilization Opportunities for Improvement: ACE Inhibitors on discharge for patients with Ejection Fraction < 40% Decreasing LOS and readmission rate Standardizing patient education materials Medical and Nursing Staff Education California Pacific Medical Center
Ace Inhibitor on Discharge for EF < 40% California Pacific Medical Center
Strategies • CNS patient population oversight • CHF patient education materials • Weight chart • One page - Tips for managing at home • CHF discharge sheet California Pacific Medical Center
Strategies for Improvement • Staff education • CNS follows CHF inpatients • Chart alert to MD - document reason no ACE prescribed • Data posted in MD newsletter, MD lounge, cardiology unit. • Data reported to Cardiology & Medicine & Nursing QA Committees. California Pacific Medical Center
California Pacific Medical CenterPermanent Pacemaker Analysis 2002 Ann Edmonson RN, Quality Improvement Jill Ley RN, Cardiac Surgery Evelyn Taverna RN, Cardiology James Mailhot MD, Cardiology QI Chair California Pacific Medical Center
Pacemaker Project • Indications • Pacer type • Vendor • Anesthesia type • Duration of procedure • Complications California Pacific Medical Center
Data Collection Processes • Softmed Report for ICD-9 Code 37.83 • Dates: Jan, 2000 – May, 2002 • Data collection methods by LOS • If LOS > 1 day – medical record review • If LOS = 1 day – PCIS review • OP note, d/c summary, blood orders • Anesthesia type and OR time not recorded • Readmission screen for all patients California Pacific Medical Center
Indications for Pacemaker # of patients California Pacific Medical Center
Pacemaker Complications • Lead Dislodgement • Infection • Pneumothorax • PM Tachycardia • Hypotension • Reprogramming • Bleeding • RV Perforation • CVA • Death California Pacific Medical Center
CNS Contributions • Ideally positioned to influence team • Knowledgeable about evidence based practices • Impact both processes and outcomes of care • Improved outcomes documented: • Reduced LOS, complication rates • Appropriate use of resources • Documented cost savings • Links to quality improvement & credentialing California Pacific Medical Center
Achieving Continual Improvement • Format meetings and forums to continually review care delivery • Implement systems to obtain data: retrospective, concurrent, prospective • Continually monitor defined indicators • Multidisciplinary reviews - close the loop • Determine when to move on to the next project California Pacific Medical Center
Clinical Nurse Specialist • Ability to Blend • clinical, research & financial aspects of outcomes management • with a focus on quality, compassion & caring. California Pacific Medical Center