Obstetric Forceps: Types, Uses, and Complications in Operative Delivery
320 likes | 501 Views
Learn about obstetric forceps, including types, uses, indications for forceps delivery, prerequisites, complications, and comparison with vacuum extractors in operative deliveries.

Obstetric Forceps: Types, Uses, and Complications in Operative Delivery
E N D
Presentation Transcript
OPERATIVE DELIVERY Rukset Attar, MD, PhD Department of Obstetrics and Gynecology
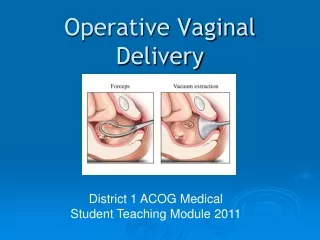
Operative Delivery • refers to an obstetric procedure in which active measures are taken to accomplish delivery • can be divided into operative vaginal delivery and cesarean delivery • Forceps • Vacuum Extraction • Cesarean section
Obstetric Forceps • Obstetric forceps is an instrument designed to assist with delivery of the baby's head. • The primary functions of the forceps are • to assist with traction of the fetal head and/or • to assist with rotation of the fetal head to a more desirable position.
Obstetric Forceps • Simpson or Elliot forceps are most often used for outlet vaginal deliveries, whereas Kielland or Tucker-McLane forceps are used for rotational deliveries. • Piper forceps are used in the United States for delivery of the aftercoming head. • The pelvic and cephalic curve, shank, blade, lock, and handle are different for each type of forceps
Obstetric Forceps • Piper forceps, which are specifically designed for breech deliveries, have a reverse pelvic curve compared to other forceps. • Simpson forceps are suited for application to the molded fetal head • Tucker-McLane forceps or Kielland forceps are more appropriate for application to the fetal head with little or no molding
Indications for forceps delivery • nonreassuring fetal heart rate pattern • shortening of the second stage of labor for fetal or maternal reasons • prolonged second stage of labor not due to dystocia • In a nulliparous patient - more than 3 hours with a regional anesthetic/more than 2 hours without a regional anesthetic. • In a multiparous patient - more than 2 hours with a regional anesthetic or more than 1 hour without a regional anesthetic. • delivery of the aftercoming head in a breech presentation.
Prerequisites for a forceps-assisted vaginal delivery • In order for a patient to be considered a candidate, all of the following must be met: • complete cervical dilatation • ruptured membranes • vertex presentation • fetal head engaged with the fetal head position known • empty bladder • no evidence of cephalopelvic disproportion • adequate analgesia • cesarean section capability and • an experienced operator
The classification of forceps • Outlet forceps is the application of forceps when • the fetal scalp is visible at the introitus without separating the labia, • the fetal skull has reached the pelvic floor, • the sagittal suture is in the anteroposterior diameter or in the right or left occiput anterior or posterior position, and the fetal head is at or on the perineum. • According to this definition, rotation of the fetal head must be equal to or less than 45 degrees.
The classification of forceps • Low forceps is the application of forceps • when the leading point of the fetal skull is at station +2 or greater and • not on the pelvic floor. • Low forceps have two subdivisions: • rotation less than or equal to 45 degrees and • rotation greater than 45 degrees. • Midforcepsis the application of forceps when the head is engaged but the leading point of the fetal skull is above station +2.
Complications • Maternal complications include • lacerations of the vagina and cervix • episiotomy extensions involving third- and fourth-degree lacerations • pelvic hematomas • urethral and bladder injuries • uterine rupture • blood loss and the need for blood transfusion are increased in forceps deliveries.
Neonatal complications • minor facial lacerations • forceps marks, • facial and brachial plexus palsies, • cephalhematomas, • skull fractures, • intracranial hemorrhage, and • seizures.
Vacuum Extractor • the indications for vacuum use are similar to those of forceps. • the classification of forceps deliveries is the same classification used for vacuum deliveries, and the prerequisites are similar.
Contraindications for vacuum delivery • place the cup directly over the sagittal suture at the median flexion point located approximately 3 cm anterior to the posterior fontanelle • approximately 600 mmHg at the beginning of a uterine contraction. • If more than 1 contraction is necessary, the vacuum pressure can be decreased to low levels between contractions.
Contraindications for vacuum delivery • While the fetal head is delivering, the cup should assume a 90-degree orientation to the horizontal as the head is extended. • Once the head has completely delivered through the vagina, the suction is withdrawn and the cup removed
Contraindications for vacuum delivery • face presentation, • breech presentation, • true cephalopelvic disproportion, • congenital anomalies of the fetal head (eg, hydrocephalus), • gestational age less than 34 weeks or • estimated fetal weight less than 2000 g, • estimated fetal weight greater than 4000 g, and • an unengaged fetal head.
Complications • neonatal • retinal hemorrhage -most common-50%-rarely has any clinical significance. • Cephalhematoma involves bleeding beneath the periosteum and complicates approximately 6% of all vacuum deliveries. • Subgaleal hematoma, a more serious complication, occurs in 50 of 10,000 vacuum deliveries-bleeding occurs in the loose subaponeurotic tissues of the scalp - there is the potential for life-threatening hemorrhage-The subgaleal space actually extends from the orbits of the eyes to the nape of the neck. This potential space can occupy over half of a newborn's blood volume. • Intracranial hemorrhage occurs in approximately 0.35% of vacuum deliveries. It can be a catastrophic complication that includes subdural, subarachnoid, intraventricular, and/or intraparenchymal hemorrhage.
Cesarean Section • A cesarean section refers to the delivery of a fetus, placenta, and membranes through an abdominal and uterine incision. • The first documented cesarean section on a living person was performed in 1610. The patient died 25 days later.
Cesarean Section • Abdwallinsitiontransverse (Pfannenstiel) incision • Classical cesarean section • is the simplest to perform. • is associated with the greatest loss of blood and may result in uterine rupture with subsequent pregnancies • accepted indications for classical cesarean section are placenta previa, transverse lie (especially back down), and preterm delivery in which the lower uterine segment is poorly developed • A classical cesarean section may be preferred if extremely rapid delivery is needed
Cesarean Section • low-transverse uterine incision • Lessblood loss • Lessfrequentlyresult in uterine rupture with subsequent pregnancies
Cesarean Section • Maternal indications • repeat cesarean delivery; • obstructive lesions in the lower genital tract including malignancies, • large vulvovaginal condylomas, • obstructive vaginal septa, and • leiomyomas of the lower uterine segment that interfere with engagement of the fetal head; and • pelvic abnormalities that preclude engagement or interfere with descent of the fetal presentation in labor.
left heart valvular stenosis, • dilated aortic valve root, • certain cerebral AVMs, and • recent retinal detachment. • Women with a prior vaginal or perineal reparative surgery, such as colporrhaphy and repair of major anal involvement from inflammatory bowel disease
Fetal indications • Malpresentation • Twin gestations • Congenital anomalies: fetal neural tube defects hydrocephalus with an enlarged biparietal diameter, and some skeletal dysplasias such as type III osteogenesis imperfecta. a fetal abdominal wall defect (ie, gastroschisis and omphalocele • Fetal distress • Maternal infections • Human immunodeficiency virus infections
Abnormal placentation, • Abruptio placenta • Cord prolapsus or presentation • Transvers presentation • Oblique presentation • Breech presentation
most common complications that result from cesarean section are • postpartum hemorrhage, • endometritis, and • wound infection.