Download
1 / 15
160 likes | 323 Views
Explore the importance of spontaneous reporting systems, strengths, limitations, evidence for causal relationships, and various approaches to causality assessment. Case examples and drug withdrawal impacts are discussed.

E N D
Challenges in Causality Assessment in Spontaneous Reporting Systems Syed Rizwanuddin Ahmad, MD, MPH, FISPE, FCP 3rd ICIUM, Antalya, Turkey November 2011
Disclaimer • These are my personal views not shared by the U.S. FDA or the U.S. government • I am not representing the FDA • No conflict of interest to declare
Outline • Spontaneous Reporting Systems • What • Why • Strengths/Limitations • Evidence to Suggest Causal Relationship • Approaches to Causality Assessment • WHO-UMC • Naranjo • Bradford Hill • Case example • Safety-related Drug Withdrawals • Conclusions
What is Spontaneous Reporting? • The process of reporting of all unsolicited reports of adverse events from health care professionals or consumers to the FDA (or any appropriate authority) is called spontaneous reporting -Ahmad SR, Goetsch RA, Marks NS. Spontaneous reporting in the United States. Chapter 9. In Strom’s Pharmacoepidemiology, 2005 p. 135-159.
Why Spontaneous Reporting? Limitations of Pre-marketing Clinical trials • Too small --- 2,000-5,000 • Too short --- <1 yr of exposure • Too narrow --- restricted population
Spontaneous Reporting –Strengths/Limitations Strengths • Inexpensive/All patients/drugs • Generation of hypothesis and signals • Good for identifying rare, serious drug-induced events with low background rate Limitations • Passive surveillance • Adverse event recognition • Underreporting • Duplicate reporting • Report quality • Reporting biases
Factors to Consider in Causal Assessment • Temporally associated with use of drug • Biological plausible • No other likely causes • Underlying diseases or disease progression • Concurrent meds • Event abates after drug is stopped (+ dechallenge) • Event recurs when drug is restarted (+ rechallenge)
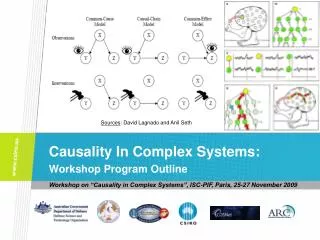
Approaches to Causality Assessment • Expert Judgement • individual assessments • no standardized tool • Algorithms • sets of specific questions with or without scores • Probabilistic or Bayesian methods • Is based on assigning a prior probability to an event of interest Agbabiaka TB, et al. Methods for causality assessment of ADRs. Drug Safety 2008;31: 21-37 Jones JK. Determining causation from case reports. In Pharmacoepidemiology, Strom BL. 2000, p. 525-538.
WHO UMC Causality Categories • Certain • Probable/Likely • Possible • Unlikely • Conditional/Unclassified • Unassessable/Unclassifiable
Bradford-Hill Criteria • Strength • Consistency • Specificity • Temporality • Biological gradient • Plausibility • Coherence • Experimental evidence • Analogy
Case Example -Exenatide and Pancreatitis A 64-year-old, nonalcoholic woman with NIDDM presented with a 1-month history of epigastric pain beginning 2 days after starting exenatide. Serum lipase concentration was 2700 U/L (reference range, 114–320 U/L), and serum amylase concentration was 131 U/L (reference range, 30–110 U/L). Liver function test results, lipid profile, and serum creatinine concentration were normal. Abdominal computed tomography (CT) showed changes consistent with pancreatitis, and the gallbladder was absent. Exenatide was discontinued. Conservative therapy resulted in rapid resolution of symptoms, normal lipase concentration (151 U/L), and normal findings from CT of the pancreas 90 days later. Ayoub W., et al. Exenatide-induced Acute Pancreatitis. Endocrine Practice. 2010;16(1):80-83.
Case Example -Exenatide and Pancreatitis - 2 • A search in FDA’s AERS database to identify additional cases of AP in association with exenatide and other antidiabetics • Reporting rate was compared with the RR of comparator antidiabetics • Reporting rates are typically based on case counts divided by some measure of drug’s utilization • If reporting rate of an event is > than background rate we can say that there is a potential association between the drug & AE • Reporting rate for exenatide was higher compared to other antidiabetics labeling change -Ahmad SR, Swann J. N Engl J Med 2008;358:1971-2. -Graham DJ, Ahmad SR, Piazza Hepp TD. Spontaneous Reporting – USA. Pp. 237-247. In: Mann R, Andrews E. (eds.). Pharmacovigilance. 2nd ed. 2007 -Ahmad SR, Graham DJ. Exenatide and acute pancreatitis: Time to event analysis. Pharmacoepidemiol Drug Saf 2008;17:S132-3. -Ahmad SR, Swann J. Reporting rates of hemorrhagic/necrotizing pancreatitis (HNP) in association with selected newer antidiabetics. Pharmacoepidemiol Drug Saf 2009;18:S79-80.
Conclusions • Spontaneous reporting systems are the most common methodology used to generate and detect new and rare signals • In spite of challenges in causality assessment, AE reports submitted to spontaneous reporting systems have been instrumental in most safety-related drug withdrawals and labeling changes