Download
1 / 29
300 likes | 658 Views
FEVER WITHOUT LOCALIZING SIGNS. Dr. bahareh vard Bahareh_vard@yahoo.com. FEVER WITHOUT LOCALIZING SIGNS. Fever of acute onset, with duration of <1 wk and without localizing signs , is a common diagnostic dilemma in children <36 mo of age. The

E N D
FEVER WITHOUT LOCALIZING SIGNS Dr. bahareh vard Bahareh_vard@yahoo.com
FEVER WITHOUT LOCALIZING SIGNS • Fever of acute onset, with duration of <1 wk and without localizing signs, is a common diagnostic dilemma in children <36 mo of age. The • etiology and evaluation of fever without localizing signs depends on the age of the child.
FWLS Traditionally, 3 age groups are considered: • neonates or infants to 1 mo of age • infants >1 mo to 3 mo of age • children >3 mo to 3 yr of ge
A 13days neonate refer to the hospital with history of 38.4 temperature in two days ago ? ? ?
Neonate • Neonates who experience fever without focus are a challenge to evaluate because they display limited signs of infection, making it difficult to clinically distinguish between a serious bacterial or viral (herpes simplex virus [HSV]) infection and self-limited viral illness.
neonates • neonates who have a fever and do not appear ill have a 7% risk of having a serious bacterial infection. • Serious bacterial infections include bacteremia, meningitis, pneumonia, osteomyelitis, septic arthritis, enteritis, and urinary tract infections. • Although neonates with serious infection can acquire community pathogens, they are mainly at risk for late-onset neonatal bacterial diseases (group B streptococci, E. coli, and Listeria monocytogenes) and perinatallyacquired herpes simplex virus (HSV) infection.
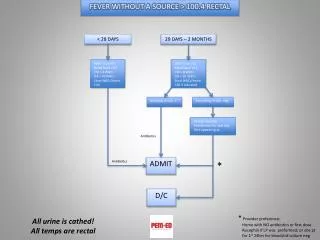
febrile neonate • if a neonate has had a fever recorded at home by a reliable parent, the patient should be treated as a febrile neonate. • If excessive clothing and blankets encasing the infant are suspected of falsely elevating the body temperature, then the excessive coverings should be removed and the temperature retaken in 15-30 min.
febrile neonate • should be hospitalized • blood, urine, and CSF should be cultured, • should receive empirical intravenous antibiotics • Stool culture and chest radiograph may also be part of the evaluation.
Empiric antibiotic therapy • ampicillin and cefotaxime or ampicillin and gentamicin • Acyclovir should be included if HSV infection is suspected because of seizures,hypotension, transaminase elevation, CSF pleocytosis, or known maternal history of genital HSV, especially at the time of delivery.
A 2mo years old boy refers to the hospital with fever (38.8 T) and appears well ????
1 to 3 Months of Age • The large majority is viral syndrome. • In contrast to bacterial infections, most viral diseases have a distinct seasonal pattern: RSV and influenza A virus infections are more common during the winter enterovirus and parechovirus infections usually occur in the summer and fall
Pyelonephritis is the most common serious bacterial infection in this age group and is also more common in uncircumcised infant boys and infants with urinary tract anomalies. is the most common and may be seen in well-appearing infants who have fever without a focus or in those who appear ill. Urinalysis may be negative in infants <2 mo of age with pyelonephritis
BACTERIAL INFECTION • E. coli is the most common pathogen identified in bacteremic infants, the majority having pyelonephritis. • Group B Streptococcus followed by S. aureus are the next most frequently identified pathogens causing bacteremia; • pneumococcus tends to be seen in older infants. • Other potential bacterial diseases in this age group include otitis media, pneumonia, omphalitis, mastitis, and other skin and soft tissue infections
Ill-appearing (toxic) febrile infants 3 mo of age or younger • hospitalization • cultures of blood, urine, and CSF • immediate parenteral antimicrobial therapy Ampicillin (to cover L. monocytogenes and Enterococcus) plus either ceftriaxone or cefotaxime • Vancomycin is added if meningitis is suspected
Infants 1-3 mo of age with fever who appear generally well with T of ≥38°C • CBC • Blood culture • LP • Stool studies if diarrhea • Urine analysis and culture • CXR
Infants 1-3 mo of age with fever who appear generally well • who have been previously healthy; • who have no evidence of skin, soft tissue, bone, joint, or ear infection; • who have a peripheral white blood cell (WBC) count of 5,000-15,000 cells/µL • absolute band count of <1,500 cells/µL, • normal urinalysis : negative leukocyte esterase, nitrite and <10 WBC/HPF • negative culture (blood and urine) results are unlikely to have a serious bacterial infection. • Stool studies if diarrhea (no RBC and <5 WBC/HPF) • CSF cell count (<8 WBC/μL) and negative Gram stain • Chest radiograph without infiltrate
The decision to obtain CSF studies in the well-appearing 1-3 mo • depends on the decision to administer empirical antibiotics. • If close observation without antibiotics is planned, a lumbar puncture may be deferred. • If the child deteriorates clinically, a full sepsis evaluation should be performed, and intravenous antibiotics should be administered • If empirical antibiotics are initiated, CSF studies should be obtained, preferably before administering antibiotics.
A 2years old daughter refers to the hospital with fever(38.5) and appears well ????
3 to 36 Months of Age • Viral infections are the cause of the vast majority of fevers in this population, but serious bacterial infections do occur and are caused by the same pathogens listed for patients 1-3 mo of age. • H. influenzae type b was an important cause of occult bacteremia in young children before universal immunization with conjugate Hib vaccines and remains common inunderdeveloped • countries that have not implemented these vaccines in their immunization schedule.
Risk factors • Risk factors indicating increased probability of occult bacteremia include temperature ≥39°C (102.2°F), WBC count ≥15,000, elevated ESR and CRP and band cell
Well appeared 3_36 mo • temperature 38-39°C : Reassurance that diagnosis is likely self-limiting viral infection, but advise return with persistence of fever, temperatures >39°C and new signs and symptoms • Child 3-36 Mo and temperature >39°C (102.2°F) Two-step process: Determine immunization status If received conjugate pneumococcal and Haemophilus influenzae type b vaccines, obtain urine studies for all girls, all boys <6 mo old, all uncircumcised boys <2 yr, all children with recurrent urinary tract infections: urine analysis and culture If did not receive conjugate pneumococcal and H. influenza type b vaccines, manage according to the 1993 Guideline
For nontoxic-appearing infants with a rectal temperature of ≥39°C options include: • obtaining a blood culture and CBC and administering empirical antibiotic therapy (ceftriaxone, a single dose of 50 mg/kg, not to exceed 1 g); if the WBC count is >15,000/μL, • obtaining a blood culture and beginning empirical ceftriaxone • obtaining a blood culture and observing as outpatients without empirical antibiotic therapy, with return for reevaluation within 24 hr.
blood culture • S. pneumoniae : • the child should return to the physician as soon as possible • If the child appears well, is afebrile, and has normal physical exam, a second blood culture should be obtained and the child should be treated with 7-10 days of oral antimicrobial therapy.
BLOOD CULTURE If the child appears ill and continues to have fever with no identifiable focus of infection at the time of follow-up, or if H. influenzae or N. meningitidis : • repeat blood culture • be evaluated for meningitis (including LP) • receive treatment in the hospital with appropriate intravenous antimicrobial agents
If the child develops a localized infection • treatment should be directed toward the likely pathogens
A 13days neonate refer to the hospital with history of 38.4 temperature in two days ago • should be hospitalized • blood, urine, and CSF should be cultured, • should receive empirical intravenous antibiotics ± acyclovir
A 2mo years old boy refers to the hospital with fever (38.8 T) and appears well • CBC • Blood culture • LP • Urine analysis and culture
A 2years old daughter refers to the hospital with fever(38.5) and appears well • Reassurance that diagnosis is likely self-limiting viral infection • but advise return with persistence of fever, temperatures >39°C and new signs and symptoms