Download

1 / 30
300 likes | 492 Views
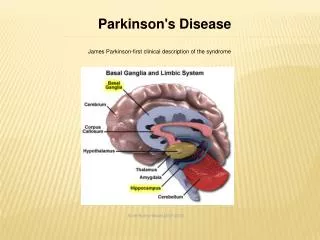
Parkinson's disease (PD). second most common age-related neurodegenerative disorder clinical symptoms, motor symptoms Nonmotor symptoms. Nonmotor Symptoms in Parkinson's disease. The Dark Side of the Moon.

E N D
Parkinson's disease (PD) • second most common age-related neurodegenerative disorder • clinical symptoms, motor symptoms Nonmotor symptoms
Nonmotor Symptoms in Parkinson's disease The Dark Side of the Moon
Nonmotor Symptoms P.D • Depression • Anxiety • Psychosis • Dementia • FATIGUE • Sleep Dysfunction • Autonomic Dysfunction • Sensory Dysfunction
Depression • Common ( 7 to 76%) • may represent the first manifestation of PD • comparison with patients without PD:anxiety pessimism irrationality suicidal ideation • higher frequency of MDD in patients with akinetic-rigid subtype when compared with a tremor-dominant • It is still controversial whether Depression has been associated with a worse motor progression
Treatment • There is no clear consensus regarding the use of antidepressants for the treatment of depression in patients with PD • the antidepressant effect of PD therapy has to be evaluated before adding specific antidepressive therapy • Dopamine agonists reduce depression in PD Pramipexole demonstrated to have the same efficacy ofSSRIin MDd beneficial effect on mood and motivational symptoms in PD patients without depression Ropinirole reduce depression • MAO)-B inhibitors weak antidepressant properties
TCAs effective in treating depression not well tolerated due to anticholinergic side effects SSRI effective in treating depression potentially serotonin syndrome aggravating motor symptoms recent studies evidenced that SSRIs only rarely aggravate motor symptoms in PD, and that sertraline may be the least mirtazapine(presynaptic α2-antagonist) effective in treating depression demonstrated in reducing Parkinsonian tremor
drug selection should be based on potential advantages versus potential side effects.
Anxiety • affects nearly 40% of patients with PD • The most common anxiety disorders in PD are panic attacks (especially during off-periods) • Benzodiazepines should be used cautiously because they may increase adverse effects • Buspirone, with dopaminergic effects, is well tolerate 10 – 40 mg
Psychosis • The most common type of psychotic symptoms in PD are hallucinations(visual)and delusions (paranoid) • Hallucinations in treated PD patients is 15–40% • Delusions occur in up to 10% of patients. • when the hallucinations occur early in the course of the disease, especially without any dopaminergic treatment, a diagnosis of levy body disease should be considered.
treatment • Excluding general causes of hallucination/confusion(fever & metabolic dysfunction & drug) • Reducing the dose or the number of antiparkinsonian drug anticholinergic drugs amantadine (COMT) inhibitors dopamine agonists Levodopa • Atypical antipsychotics • Cholinesterase inhibitors
Atypical antipsychotics Clozapine and quetiapine do not appear to worsen parkinsonism as do other atypical , and the typical neuroleptics clozapine is the only atypical antipsychotic fully recommended for the treatment of psychosis in PD. because of the side effect of agranulocytosis, which requires frequent blood testing Quetiapine represents the most commonly used antipsychotic treatment in PD patients.
Cholinesterase inhibitors rivastigmine, the only cholinesterase inhibitor that is US FDA-approved for the treatment of dementia in PD, demonstrated an improvement in neuropsychiatric symptoms in PD patients with dementia
Dementia • higher risk of developing dementia 30 -40% • mean duration of PD before diagnosis of dementia is 10 years • subtle cognitive deficits can be identified in the early stages • Risk factors for PD–D include: age visual hallucinations severe motor symptoms : rigidity postural instability gait disturbances
Management of dementia in PD • systematic assessment • Anticholinergics, amantadine and benzodiazepines should be avoided because of their relationship with a reduction in cognitive performances. • Dopamine agonists should be used cautiously • Cholinesterase inhibitors
Cholinesterase inhibitors donepezil and rivastigmine have been demonstrated to significantly improve cognitive impairment memantine, can improvement of cognitive symptoms, even if its triggering effect on psychosis may limit the use in clinical practice.
FATIGUE • Fatigue is a common problem in patients with Parkinson disease • Treatment of fatigue in PD begins with an attempt to identify the cause. Excessive daytime sleepiness and depression are both the most common and the most treatable identifiable causes. • True fatigue unassociated with sleepiness or depression is more difficult to treat • Suboptimally treated bradykinesia sometimes presents as subjective fatigue • Medications used for empiric treatment of fatigue, such as amantadine and stimulants, such as methylphenidate
Sleep Dysfunction • Sleep dysfunction 75 to 98% in the PD population Disorders of sleep initiation and maintenance Excessive daytime sleepiness (EDS) Sleep attack (SA) Rapid eye movements behavior disorder (RBD )
Disorders of sleep initiation and maintenance • Sleep fragmentation, the most common manifestation • characterized by reduction in the stages III/IV or REM sleep • could be due to : motor manifestations of PD, such as o dystonia and cramp bladder dysfunction, such as nocturia. Restless-legs syndrome (RLS) Sleep apnea
Treatment should include • good sleep hygiene • Improved control of motor symptoms of PD • Treatment of RLS (dopaminergic agents) • Hypnotic agents is not first line for potential side effects, specifically confusion and daytime sleepiness. • There are no controlled data on any specific hypnotic agent in PD • Ramelteon, a new hypnotic agent approved for sleep initiation insomnia, which is a ligand of melatonin receptors, may be useful in PD ( 8 mg orally once a day, 30 minutes prior to bedtime)
Excessive daytime sleepiness (EDS) • very common among patients with PD, up to 50% • Factors that contribute to EDS is motor disability, nocturnal sleep impairment depression and dementia, • higher prevalence of somnolence in patients treated with dopamine agonists • modafinil has not been effective for treating drowsiness in patients with PD.
Sleep attack (SA) • sleepiness that occurs without warning • Patients may be unaware of prodromal sleepiness • dopaminergic drugs provoke excessive daytime sedation
Rapid eye movements behavior disorder (RBD ) • prevalence in PD patients ranges between 33 and 60% • male > female this male predominance are not yet known • treated with clonazepam in small doses (0.25–1 mg) dopaminergic agents (DA , levodopa) donepezil Melatonin was reported to be effective at doses of 3–12 mg.
Autonomic Dysfunction • Cardiovascular Dysfunction • Gastrointestinal Symptoms • Urinary & Sexual Dysfunction • Hyperhydrosis
Cardiovascular Dysfunction • PD patients have higher BP at the off-stage than at on-stage • patients with the on–off type of motor fluctuation have higher resting heart rate, greater orthostatic BP • Early diagnosis and symptomatic treatment of orthostatic hypotension can greatly improve quality of life and, improve cardiovascular mortality
Treatment • reduction of dopamine agonists is often necessary • Domperidone, a peripheral dopamine-blocking agent • reduction of antihypertensive drug • increase BP α-adrenergic agents such as midodrine salt-retaining mineralcorticoids (e.g., fludrocortisone). Pyridostigmine was reported to be effective in neurogenic orthostatic hypotension but has not been specifically tested in PD.[ Nonpharmacological elevation of the head of the bed by 10–30°, increase in salt and fluid intake and the use of waist-high compression stockings.
Gastrointestinal Symptoms • Constipation exercise, dietary modifications, increases in fluid intake and ultimately use of laxatives (Psyllium, bisacodyl) coexistent abdominopelvic dyssynergia could be worsened by the use of laxatives recalcitrant constipation neostigmine, symbiotic yogurt containing components, botulinum toxin injections and sacral nerve stimulation. Dysphagia the risk of food inhalation no evidence of increased survival in patients receiving enteral tube feeding.
Nausea often due to dopamine replacement therapy adjustment of the timing of levodopa therapy in relation to food and the use of domperidone. Hypersalivation reduced ability to swallow rather than overproduction of saliva Anticholinergics and injection of botulinum toxin into the salivary glands are therapeutic option
Urinary & Sexual Dysfunction • Patients usually develop detrusor muscle hyperactivity • Oxybutynin and tolterodine memory loss and constipation, must be taken into consideration • Sexual dysfunction: male erectile dysfunction .60% of PD • Sildenafil citrate has been found to be safe and effective
Hyperhydrosis • related to hypothalamic dysfunction • Treatment options for hyperhydrosis are limited.Propranolol has been helpful in some cases.