Download
1 / 17
190 likes | 529 Views
Right Internal Jugular Central Vein Catheterization. A Course for Emergency Department Rotators. Updated 11/3/11 M Zwank, MD. INDICATIONS. CONTRAINDICATIONS. Uncooperative patient Known IJ DVT Adequate peripheral access Bleeding diathesis. Definitive access in difficult access patients

E N D
Right Internal JugularCentral Vein Catheterization A Course for Emergency Department Rotators Updated 11/3/11 M Zwank, MD
INDICATIONS CONTRAINDICATIONS Uncooperative patient Known IJ DVT Adequate peripheral access Bleeding diathesis • Definitive access in difficult access patients • Critically ill patients needing multiple infusions • Central vein infusions • ie. pressors
Equipment • Face Shield • Hair Covering (bouffant cap anyone?) • Sterile Gown • Sterile Gloves • Sterile Gloves for attending when you miss it • Central Line Kit • Ultrasound Machine, Probe Covering • Saline Flush(es)
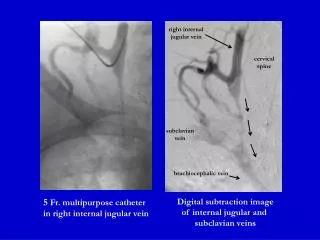
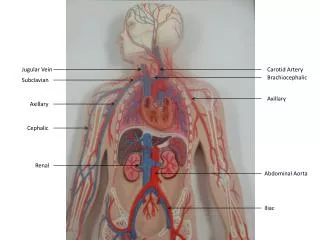
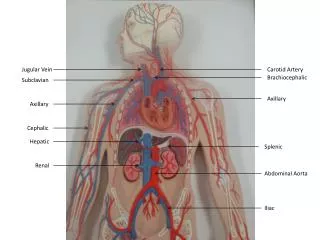
Anatomy • Multiple traditional approaches • Anterior, central (most common), posterior • IJ generally courses lateral to carotid but don’t count on it • Use ultrasound • Seriously, use ultrasound lateral medial SCM I J C
Why Bother With Ultrasound • Agency for Healthcare Research & Quality promotes it • Multiple multiple studies support it • Takes all trepidation out of procedure • Priceless
Agency for Healthcare Research & Quality 2001 • Ultrasound guidance for central line placement • Other recommendations • Venous thromboembolism (VTE) prophylaxis • Perioperative beta-blockers • Sterile barriers AHRQ. Making health care safer: a critical analysis 2001;43:i–x, 1–668.
Challenges – Internal Jugular • Anatomic Variations (Troianos) • 1009 patients admitted for surgery • 54% had internal jugular vein overlying carotid • Double wall puncture (Docktor) • 150 patients • Double wall puncture in 30 Troianos CA, et al. Anesthesiology 1996; 85:43–8; Docktor B, et al. Can Assoc Radiol J 1996;47: 195–201.
Universal Protocol ! ! ! • Guidelines intended to prevent procedure errors • Wrong Site • Wrong Procedure • Wrong Person • Required by JCAHO • Currently applicable to several ED procedures • Central Line, LP, Thora/Paracentesis, Chest Tube • Includes three major steps
Universal Protocol Three Steps • The verification processes to confirm • Correct Patient • Correct Procedure • Correct Site • The marking of the procedure site • A “time-out” immediately before starting the procedure
Procedure • Consent if possible • Prep • Perform • Confirm
Prep • Gather everything, Relax, Clear your head • Ultrasound machine on • Patient in trendelenburg • Wash hands • Head covering, face covering, gown, gloves • Open kit • Sterile Prep and Drape
Perform • Prepare items to be used • Flush and clamp ports • Locate vein with ultrasound • Anesthetize skin and tissue • Needle to vein, be careful of tenting vein • Get flash of blood, hold needle still
Perform • Wire • Rotate wire and/or needle 90° if trouble wiring • Skin nick (be generous) • Dilate tissue to vein • Catheter over wire • Draw and flush ports • Secure with suture • Secure line • Apply sterile dressing
Confirm • Generally CXR • Consider Ultrasound • Agitated saline injected will be seen in R atrium / ventricle on ultrasound
Cautions • Stop if you break sterile technique • Don’t sweep needle when in tissue • Never let go of guidewire • Don’t force guidewire • Watch for cardiac ectopy if wire is too deep • Stop procedure if arterial stick • Clean up your sharps after!
Video http://www.nejm.org/doi/full/10.1056/NEJMvcm055053 Start video at Chapter 4; 6:10