Download
1 / 2
30 likes | 149 Views
May 2010. Pathway for the referral of patients with suspected cardiac arrhythmia, cardiac syncope or SCD (guidance notes on back). History, Examination, Pulse palpation, ECG , +/- Echo. Transient palpitations Clear evidence of vasovagal symptoms (1). Suspected AF Confirmed by abnormal ECG.

E N D
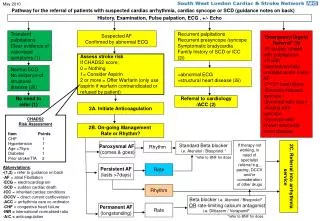
May 2010 Pathway for the referral of patients with suspected cardiac arrhythmia, cardiac syncope or SCD (guidance notes on back) History, Examination, Pulse palpation, ECG , +/- Echo Transient palpitations Clear evidence of vasovagal symptoms (1) Suspected AF Confirmed by abnormal ECG Recurrent palpitations Recurrent presyncope /syncope Symptomatic bradycardia Family history of SCD or ICC (2i) Emergency/Urgent Referral* (3) -Pt acutely unwell with palpitations -Pt with haemodyanically unstable acute onset AF -2nd/3rd heart block -Exercise induced syncope -Syncope with injury -Angina with syncope -Syncope with known structural heart disease Assess stroke risk If CHADS2 score; 0 = Nothing 1= Consider Aspirin 2 or more = Offer Warfarin (only use aspirin if warfarin contraindicated or refused by patient) Normal ECG No evidence of structural disease (2ii) +abnormal ECG +structural heart disease (2ii) No need to refer (1) Referral to cardiology /ACC (2) 2A. Initiate Anticoagulation CHADS2 Risk Assessment Item Points CHF 1 Hypertension 1 Age >75yrs 1 Diabetes 1 Prior stroke/TIA 2 2B. On-going Management Rate or Rhythm? If therapy not working, in need of specialist referral e.g., pacing, DCCV and/or consideration of other drugs Paroxysmal AF (comes & goes) Rhythm Standard Beta blocker i.e. Atenolol / Bisoprolol * *refer to BNF for dose • Abbreviations; • -(1,2) = refer to guidance on back • AF = atrial Fibrillation • ECG = electrocardiogram • SCD = sudden cardiac death • ICC = inherited cardiac conditions • DCCV = direct current cardioversion • ACC = arrhythmia care co-ordinator • CHF = congestive heart failure • INR = international normalised ratio • A/C = anticoagulation Persistent AF (lasts >7days) Rate 2C. Referral into arrhythmia service Rhythm Beta blocker i.e. Atenolol / Bisoprolol* OR rate-limiting calcium antagonist i.e. Diltiazem / Verapamil* Permanent AF (longstanding) Rate *refer to BNF for dose
Pathway guidance for the referral of patients with suspected cardiac arrhythmia, cardiac syncope or SCD 1) ‘Green’ patients considered manageable in primary care. Clear evidence of vasovagal symptoms is suggested by young age, recurrent symptoms particularly with a known precipitant, e.g., cough, micturition, anxiety or crowded hot spaces. If in doubt or symptoms persist consider cardiology referral or to ACC for reassurance. 2) ‘Amber’ patients – first line treatment should be considered in primary care. 2i)In cases of SCD in those <35yrs, screening of family members is indicated. Consider referral to genetic arrhythmia clinic or similar specialist service. Liaison with the ACC is recommended. 2ii)History of structural heart disease might include; history of MI, cardiomyopathy, valvular heart disease, cardiac failure, or left ventricular hypertrophy. 2A. Anticoagulation – in cases of previously unknown AF consider initiation of anticoagulation. Indications for referral to secondary care anticoagulation service are; -Bleeding with high INR (urgent referral to admitting medical team) -Pregnancy (urgent referral to a/c clinic) -Planned surgical intervention (written referral to lead clinician for a/c service) -Cardioversion -Patient’s requiring treatment for active cancer (written referral to lead clinician for a/c service) If in doubt consider discussing with ACC or cardiologist prior to a referral. Consult NICE AF guidance (2006) • 2B. Rate or Rhythm? • Try Rate ControlFIRST for patients with persistent AF who are; • over 65 • with CHD • with contraindications to antiarrhythmic drugs • unsuitable for DCCV 2B. Rate or Rhythm? Try Rhythm ControlFIRST for patients with persistent AF who are; -symptomatic -younger -presenting for the first time with lone AF -secondary to treated/corrected precipitant -with congestive heart failure 2C. Referral into arrhythmia service Referral Criteria;Local secondary care team contact details; -Patient brings copy of ECG St George’s Healthcare NHS Trust - 020 8725 0744 -Acute onset stable AF Epsom and St Helier University Hospitals NHS Trust - 020 8296 3175 3) ‘Red’ patients for emergency/urgent referral– Abnormal ECG could include; evidence of previous MI or LVH, significant T wave inversion, left bundle branch block, pre-excitation (WPW syndrome), QTc interval prolongation (>460ms). Always include copy of ECG in referral unless pt is acutely unwell. History of structural heart disease might include history of MI, cardiomyopathy, valvular heart disease, cardiac failure, or ventricular hypertrophy.