Download

1 / 58
890 likes | 2.14k Views
Motor Neurone Disease. What is MND?. Regional Care Development Advisor. Colin Pearson. Motor Neurone Disease. Not contagious Not directly hereditary Is a terminal disease No cure Path of disease is different in every person

E N D
Motor Neurone Disease
What is MND? Regional Care Development Advisor Colin Pearson
Motor Neurone Disease • Not contagious • Not directly hereditary • Is a terminal disease • No cure • Path of disease is different in every person • Currently one medication that may improve quality / prolonging of life – Riluzole (Rilutek) • Onset and progression is variable – can progress swiftly with rapid deterioration • Mostly an adult Illness – most people affected are over 50 years of age
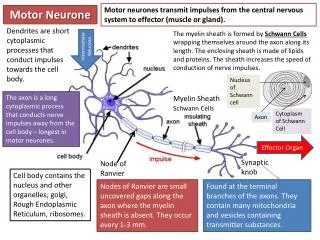
Upper motor neurones originate in the base of the cortex of the brain Lower motor neurones originate in the spinal cord Function of Motor Neurones
Amyotrophic Lateral Sclerosis – 65% • Upper and lower motor neurones affected • Spasticity (stiffness) • Muscle weakness – often develops in hands and feet first • Brisk reflexes
Progressive Bulbar Palsy – 25% • Affects bulbar muscles which control speech, swallowing and chewing • Gradual loss of speech • Swallowing problems – food and saliva • Leads to muscle weakness – especially upper limbs/neck/shoulder
Progressive Muscular Atrophy – 10% • Lower motor neurones • Starts in small muscles of the hand • Muscle wasting • Fasciculation
Primary Lateral Sclerosis - Rare • Only upper motor neurone damage • Characterised by muscle weakness, stiffness of limbs, and increased reflex response • Affects men predominantly – twice as often as women • Onset usually after 50 years of age • Survival similar to normal lifespan
Symptoms • Muscle wasting and weakness • Fasciculation (twitching) • Cramps • Spasticity (stiffness) • Respiratory problems • Speech and swallowing problems • Saliva and mucus problems • Weight loss • Fatigue • Pain • Emotional Lability • Psycho-social aspects • Cognitive changes
Rarely affected • Senses: touch, taste, sight, smell and hearing • Bowel and bladder function • Sexual function and sexuality • Eye Muscles • Heart muscles
Causes • The cause of MND is thought to be a combination of lifestyle, environmental and genetic factors. These factors accumulate throughout a person’s life. • However, the evidence obtained in studies about the above factors has often been conflicting or circumstantial and there are no clear conclusions (e.g. High levels of exercise, mechanical trauma). • Lifestyle factors could have a cumulative effect in weakening nerve. • Although some knowledge about different factors is available the cause is basically yet unknown!
Key facts to underpin knowledge • MND is not contagious • 90% - 95% of people have the sporadic (random) form • There is however a 5 - 10% familial (genetic link) pattern • Can affect adult at any age but most are over 40 with highest numbers between 50 – 70 • Men are affected twice as often than women • Precise figures of incidence and prevalence are still uncertain. • Incidence (may develop) is approx 2 per 100,000 • Prevalence (actually have) is between 5 – 10 in 100, 000
Diagnosis • No specific test • Elimination of other causes • GP may see MND once in career • Other conditions often diagnosed first • Examination and tests required by a Consultant Neurologist • Often takes over a year to receive diagnosis
How would you change your caring routine to respond to the fatigue that a person with MND experiences? Why is it important to believe a person with MND when they say they can’t do something? Moving & Handling
MND does not usually cause incontinence. What other problems though might you encounter around continence? What issues might you encounter helping someone who can’t move on their own use the toilet? Toileting / Bathing
Where would you sit or stand? How much time would you need? Where would you look? What would you do if you didn’t understand? Communication
How would you help a person who has difficulty chewing & swallowing? What things can be done to help control saliva and excessive secretions? Eating & Swallowing
Breathlessness on exertion or lying down Poor Sleep Excessive daytime sleepiness Headaches on awakening Excessive nocturnal sweating Clues to respiratory muscle involvement in MND
MND has been traditionally viewed as a disease affecting the motor system with no compromise of cognitive abilities. Recent research shows that 25% or more show some cognitive changes in the frontal lobe region 3-5% will have fronto-temporal dementia (FTD) Cognitive Change
Characteristics of FTD Significant personality change “they are not the same person” • Disinhibition – socially undesirable, inappropriate behaviour • Impulsivity – acting without thinking. Inability to delay gratification • Perseveration – continuing to conduct activity inappropriate to present situation • Impaired verbal expression and initiation • Withdrawn – failure to initiate activities - apathy
Fatigue Social Isolation Frustration / Anger Loss of identity Inability to communicate Emotional Lability Cognitive Change Carer issues Issues to consider
MND Nurse Palliative Services Resp Service Dietician MNDA Therapy Team RCA AVs
The Mental Capacity Act 2005 came into force during 2007. A number of government departments sponsored its implementation: Ministry of Justice, the Department of Health, the Office of the Public Guardian and the Welsh Assembly Government. The MCA says that a person is unable to make a particular decision if they cannot do one or more of the following four things: understand information given to them retain that information long enough to be able to make the decision weigh up the information available to make the decision communicate their decision. Mental Capacity Act 2007
At the heart of the MCA in terms of concepts and values are the five ‘statutory principles’. Consider the five principles as the benchmark – use them to underpin all acts done and decisions taken in relation to those who lack capacity. In doing so, you will better empower and protect individuals who lack capacity. It is useful to consider the principles chronologically: principles 1 to 3 will support the process before or at the point of determining whether someone lacks capacity. Once you’ve decided that capacity is lacking, use principles 4 and 5 to support the decision-making process. Principle 1: A presumption of capacity Principle 2: Individuals being supported to make their own decisions Principle 3: Unwise decisions Principle 4: Best interests Principle 5: Less restrictive option Mental Capacity Act 2007
‘Social Care has an important role in the protection of members of the public before harm has happened and after it has happened’ (No Secrets, 2009) Those who need safeguarding help are often elderly and frail, living on their own in the community, or without much family support in care homes. Safeguarding encompasses six key concepts: empowerment, protection, prevention, proportionate responses, partnership and accountability. Social care organisations play an important role in the protection of members of the public from harm and are responsible for ensuring that services and support are delivered in ways that are high quality and safe. Safeguarding & The Vulnerable Adult
Capacity is a highly significant factor in both understanding and intervening in situations of self-neglect There are a wide range of perspectives that inform professionals’ understanding of self-neglect. There are tensions between respect for autonomy and a perceived duty to preserve health and wellbeing. The former principle may extend as far as recognising that an individual who chooses to die through self-neglect should not be prevented from doing so; the latter may engage the view that action should be taken, even if resisted, to preserve an individual’s safety and dignity. The autonomy of an adult with capacity is likely to be respected, and efforts directed to building and maintaining supportive relationships through which services can in time be negotiated. Safeguarding & Self Neglect
The Deprivation of Liberty Safeguards are an amendment to the Mental Capacity Act 2005. They apply in England and Wales only. The Mental Capacity Act allows restraint and restrictions to be used – but only if they are in a person’s best interests. Extra safeguards are needed if the restrictions and restraint used will deprive a person of their liberty. These are called the Deprivation of Liberty Safeguards. DOLS – Deprivation of Liberty Safeguard
The Deprivation of Liberty Safeguards can only be used if the person will be deprived of their liberty in a care home or hospital. In other settings the Court of Protection can be asked if a person can be deprived of their liberty. Care homes or hospitals must ask either a local authority/Northern Ireland health and social care trust or health body if they can deprive a person of their liberty. This is called requesting a standard authorisation. DOLS – Deprivation of Liberty Safeguard