Download
1 / 22
220 likes | 235 Views
This overview provides information on different types of depression, including Major Depressive Disorder, Dysthymic Disorder, and Depressive Disorder Not Otherwise Specified (NOS). It also discusses the epidemiology of depression and the common symptoms associated with each type. Additionally, two case studies are presented to help illustrate the different presentations of depression in individuals.

E N D
Depression Overview Developed by the Center for School Mental Health with support provided in part from grant 1R01MH71015-01A1 from the National Institute of Mental Health and Project # U45 MC00174 from the Office of Adolescent Health, Maternal, and Child Health Bureau, Health Resources and Services Administration, Department of Health and Human Services
Depressive Disorders • Major Depressive Disorder • Dysthymic Disorder • Depressive Disorder Not Otherwise Specified (NOS)
Depression Epidemiology • 2.5% of children, up to 5% of adolescents • Prepubertal-1:1/F:M; adolescence-4:1/F:M • Average length of untreated Major Depressive Disorder – 7.2 months • Recurrence rates-40% within 2 years • Heredity • Most important risk factor for the development of depressive illness is having at least one affectively ill parent
Depression Modifications in DSM- IV for children: • irritable mood (vs. depressive mood) • observed apathy and pervasive boredom (vs. anhedonia) • failure to make expected weight gains (rather than significant weight loss) • somatic complaints • social withdrawal • declining school performance
What type of depression?? • Tonya has come for an initial appointment to the SBHC. During the risk assessment, Tonya reports a number of depressive symptoms, including suicidal ideation. Tonya seems to display a lot of negative thinking and cognitive distortions. For example, she believes that “nobody” likes her and that she will “never” be successful in school. Her math teacher often compliments her work, but Tonya dismisses the teacher’s comments as him “just trying to be nice.” Tonya has good grades in all classes except for one, yet she only acknowledges her below average Chemistry grade. Tonya has felt extremely sad for about three weeks, which is a contrast from her usually happy disposition.
Major Depressive Disorder • Major Depressive Episode: Five (or more) of the following symptoms have been present during the same two-week period and represent a change from previous functioning. At least one symptom is either (1) depressed mood or (2) loss of interest or pleasure. • Depressed mood most of the day, nearly every day, as indicated by subjective report or based on the observations of others. In children and adolescents, this is often presented as irritability. • Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day • Significant weight loss when not dieting or weight gain (change of more than 5% of body weight in a month), or decrease or increase in appetite nearly every day • Insomnia or hypersomnia nearly every day • Psychomotor agitation or retardation nearly every day (observable by others) • Fatigue or loss of energy nearly every day • Feelings of worthlessness or inappropriate guilt nearly every day • Diminished ability to think, concentrate, make a decision nearly every day • Recurrent thoughts of death, recurrent suicidal ideation with or without a specific plan, or an actual suicide attempt
Major Depressive Disorder II. Symptoms cause clinically significant distress or impairment in social or academic functioning III. Symptoms are not due to the direct physiological effects of a substance (drugs or medication) or a general medical condition • Although there is a different diagnostic category for individuals who suffer from Bereavement, many of the symptoms are the same and counseling techniques may overlap.
What type of depression?? • Maria comes for a follow-up appointment to the SBHC. Her risk assessment showed that she has felt sad or blue for at least two weeks. Upon further inquiry, Maria reports that she generally feels sad, and finds little enjoyment in activities. She reports having felt this way for several years. In fact, she can’t recall a time when she didn’t feel mostly down. She denies suicidal ideation, and is doing pretty well in school. She is not very social, but does have a few friends.
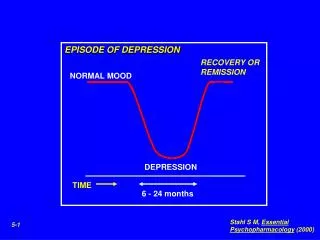
Dysthymic Disorder • Major difference between a diagnosis of Major Depressive Disorder and Dysthymia is the intensity of the feelings of depression and the duration of symptoms. • Dysthymia is an overarching feeling of depression most of the day, more days than not, that does not meet criteria for a Major Depressive Episode. • Impairs functioning and lasts for at least one year in children and adolescents, two in adults.
Depressive Disorder NOS • Disorders with depressive symptoms BUT do not meet criteria for: Major Depressive Disorder, Dysthymic Disorder, Adjustment Disorder with Depressed Mood, or Adjustment Disorder with Mixed Anxiety and Depressed Mood • Examples: premenstrual dysphoric disorder, minor depressive disorder (at least 2 weeks, but < 5 symptoms) • Also used in situations in which clinician has concluded that a depressive disorder is present, but is unable to determine whether it is primary, due to medical condition, or substance induced
Adolescent Development • Periods of transient milder problems with low self-esteem, anxiety, depressive feelings are quite common. • Needs to be differentiated from clinical depression!
Suicide • Attempts- 3:1/F:M, Completions- 4:1/M:F • Most common means of completed suicide: FIREARMS • Most often associated with depressive disorder. • Risk factors: Age, sex, presence of psychiatric illness, family history, isolation from friends, substance abuse
Adolescents and Suicide • In 1998, 4,153 young people, ages 15-24, committed suicide in the United States an average of 11.3 per day.1 • Suicide is the third leading cause of death in this age group following unintentional injury and homicide2 • Suicide accounts for 13.5% of all deaths in this age-group1 1 Murphy, SL, 1998 2 The Surgeon General’s Call to Action to Prevent Suicide, 1999
Mortality in ChildrenAges 1-19 years Source: CDC Wonder Mortality Statistics; Center for Disease Control and Prevention, 2001
MH interventions shown to be EFFECTIVE for depressive or withdrawn behavior problems • “Of the available services reviewed, Cognitive Behavioral Therapy remains the intervention of choice… Interpersonal Therapy appears to be a reasonable alternative to CBT”
What is Cognitive Behavior Therapy (CBT)? • Relatively short-term, focused psychotherapy • Focus: • How you are thinking (your cognitions) • How you are behaving and communicating • Emphasis on present rather than past • Learn coping skills
What is Interpersonal Therapy (IPT)? • Short term, usually involves up to 20 sessions • Focuses on 1-2 key interpersonal issues most closely related to the depression. • Interpersonal events include: • interpersonal disputes / conflicts • interpersonal role transitions • complicated grief
MH interventions with little or NO evidence of effectiveness for Depression: • Family Therapy* • Relaxation • Self-Control Training • Self-Modeling • Non-directive Supportive Therapy * note: Family Engagement in CBT and IPT, however, has been shown to be important!
Practice Elements for Depression • Child Psychoeducation • Cognitive/Coping • Problem Solving • Activity Scheduling • Skill-building/Behavioral Rehearsal • Social Skills Training • Communication Skills • Parent Psychoeducation