Download
1 / 41
860 likes | 2.34k Views
Exercise Prescription for Cardiovascular disease. Dr. Leung Tat Chi, Godwin Specialist in Cardiology 3 Feb 2007. Current Recommendation of PA for Health Promotion. 1996 U.S. Surgeons’ General Report: Physical Activity and Health (USDHHS / CDC / ACSM).

E N D
Exercise Prescription for Cardiovascular disease Dr. Leung Tat Chi, Godwin Specialist in Cardiology 3 Feb 2007
Current Recommendation of PA for Health Promotion 1996 U.S. Surgeons’ General Report: Physical Activity and Health (USDHHS / CDC / ACSM) • Individuals should engage in 30 minutes or more of moderate intensity physical activity on most days (preferably all) of the week • effectively reduce the risk of coronary heart disease, type 2 diabetes, hypertension, stroke and cancer of the breast and colon
Prevention of Atherosclerotic Vascular Disease by Physical Exercise • Physical activity reduces the incidence of CAD • Physical inactivity is a major CAD risk factor • The relation is strong, with the most physically active subject generally demonstrated CAD rates half those of the most sedentary group • Independent of other risk factors • Not protective in later years without lifelong physical activity • Benefit seen in middle age and older age groups Powell KE, Thompson PD, Caspersen CJ, et al. Physical activity and the incidence of coronary heart disease. Annu Rev Public Health. 1987;8:253-287
Reduction of Atherosclerotic Risk Factors • Physical activity both prevents and treats establish atherosclerotic risk factors: • Elevated blood pressure • Insulin resistance • Glucose intolerance • Elevated triglyceride concentration, low HDL-C • Obesity • Exercise + weight reduction >>>> LDL-C and increase HDL Thompson et al, Exercise and Physical Activity in Cardiovascular Disease. Circulation June 24, 2003; 107:3109-3166
Response of Blood Lipids to Exercise Training • Meta-analysis of 52 exercise training trials of >12 weeks • Include 4700 patients • Change in lipid profile • HDL-C increase 4.6% • Reduction in LDL-C by 5.0% • Reduction in TG by 3.7% Leon AS, Sanchez O. Meta-analysis of the effects of aerobic exercise training on blood lipids. Circulation. 2001;104(suppl II):II-414-415. Abstract.
Response of Blood Pressure to Exercise Training • 44 randomized controlled trials include 2674 patients • Average change in blood pressure • SBP decrease by 3.4 mmHg • DBP decrease by 2.4 mmHg • Hypertensive patient • SBP decrease by 7.4 mmHg • DBP decrease by 5.8 mmHg • Normotensive patient • SBP decrease by 2.6 mmHg • DBP decrease by 1.8 mmHg BP drop is not dose related Fagard RH. Exercise characteristics and the blood pressure response to dynamic physical training. Med Sci Sports Exerc. 2001;33(6 suppl)
Response of Insulin Resistance to Exercise Training • Physical activity reduces insulin resistance and glucose intolerance, postprandial hyperglycemia, and possibly hepatic glucose output • 9 randomized trials include 337 patients • Reports reduction of hemoglobin HbA1c of 0.5% to 1% Thompson PD, Crouse SF, Goodpaster B, et al. The acute versus the chronic response to exercise. Med Sci Sports Exerc. 2001;33(6 suppl)
Outcome Mean Difference 95% Cl Statistically Significant? Exercise-only intervention Total mortality -27% -2% to –40% Yes Cardiac mortality -31% -6% to –49% Yes Nonfatal MI -4% -31% to +35% No Comprehensive rehabilitation Total mortality -13% -29% to +5% No Cardiac mortality -26% -4% to –43% Yes Nonfatal MI -12% -30%-+12% No Effect of Exercise-based Cardiac Rehabilitation on Cardiac Events Cl indicates confidences intervals. Cls not including zero are statistically significant. • Meta analysis include 51 randomized trials • Include 8440 patients: CABG, PTCA, MI, angina, middle-age men • Supervised exercise for 6 months, follow up 2 years later Jolliffe JA, Rees K, Taylor RS, et al. Exercise-based rehabilitation for coronary heart disease. Cochrane Database Syst Rev. 2001(1):CD001800
The Exercise Training Intervention after Coronary Angioplasty • Randomised 118 patients after coronary revascularization • 6 months of exercise training vs usual care • Trained patients significant increases in peak VO2 (26%) • Quality of life parameters increases in 27% • Fewer cardiac events (11.9% vs 32.2%) • Hospital readimissions (18.6% vs 46%) • Residual coronary stenosis decrease by 30% • Recurrent cardiac event reduced by 29% BelardinelliR, Paolini I, Cianci G, et al. Exercise Training Intervention after Coronary Angioplasty: the ETICA trial. J Am Coll Cardiol., 2001;37:1891-1900
Risk • Cardiac rehab programs • Cardiac arrest: 1 in 117000 (patient-hours of participation) • Nonfatal MI: 1: in 220000 • Death : 1: 750000
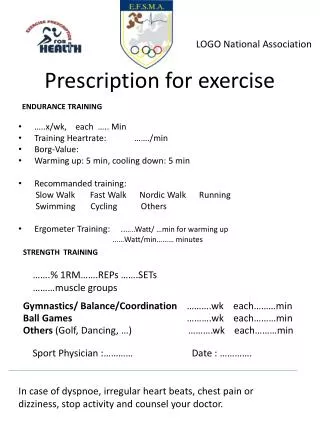
Exercise prescription for Hypertension • Follow general recommendations for aerobic exercise prescription, with slight reduction in intensity (40-70% of VO2max or HRR, i.e. 55-80% of the maximal heart rate.) The lower range of intensity is sufficient for the elderly. • 3 or 4 times weekly for at least 30 minutes at a time • Various endurance exercise modes are suitable. Resistance training (preferably circuit training) should not be the only form of exercise but should be combined with endurance training. • Emphasis on large muscle group aerobic activity. • Avoid high-intensity resistance training (lower intensity, higher repetitions). • Training at an intensity of about 50% of the maximal exercise performance (moderate-intensity) is sufficient with regard to resting blood pressure reduction (Fagard, 2001). Finnish Medical Society Duodecim. Physical activity in the prevention, treatment and rehabilitation of diseases. 2004 Apr 20
Hypertension Patients should maintain hypertensive medications, if prescribed. • Monitor blood pressure before, during, and after exercise • Unusually high blood pressures (>190mmHg systolic) during low-level activity may warrant adjustment in medical therapy • Stop when there is a 10 to 15mmHg fall in BP during exercise and further evaluation should be performed • Begin pharmacological treatment prior t starting exercise program if BP > 160/100
Cardiovascular System Assessment • Patients with known coronary artery disease should undergo a supervised evaluation of the ischemic response to exercise, ischemic threshold, and the propensity to arrhythmia during exercise. • In many cases, left ventricular systolic function at rest and during its response to exercise should be assessed. Physical Activity/Exercise and Diabetes; Diabetes care, vol. 27, supplement 1, January 2004
Exercise testing • Integral component of the rehab process • Establishment of appropriate specific safety precautions • Guide training intensity • Target exercise training heart rates • Initial levels of exercise training work rates • Risk stratification • Should be performed on all cardiac patients entering an exercise training program
Exercise prescription for individuals with CAD (Risk Stratification) • Mildly increased risk • Preserved LV systolic function (EF > 50%) • Normal exercise tolerance for age • > 50 years old > 10METS • 50 to 59 >9METS • 60 to 60 >8METS • >70 >7METS • Absence of exercise induced ischemia • Absence of hemodynamically significant stenosis of a major coronary artery (>50%) • Successful revascularization
Exercise prescription for individuals with CAD (Risk Stratification) • Substantially increased risk • Impaired LV systolic function (<50%) • Evidence of exercise-induced myocardial ischemia • Hemodynamically significant stenosis of a major coronary artery (>50%)
Eligibility recommendations for competitive athletes with cardiovascular abnormalitiesMildly increased risk CAD: IA, IIA
Medically Supervised Exercise • Moderate to High risk subjects • Class C • Medical supervision required until safety established • ECG and BP monitoring (usually > 12 sessions) • Low risk subjects • Class B • Benefit from medically supervised programs • Safe • Group dynamics • ECG monitoring (useful during the early phase, 6 – to 12 sessions) • Unmonitored exercise • For conditioning • 1 to 2 weeks post MI • Walking • Safe, low-impact, controllable
Exercise prescription for individuals with CAD • Inpatients • Walking • Active but non-resistance range-of-motion exercise of the upper extremities
Inpatient exercise program • Intensity • RPE <13 • Post MI: HR <120BPM or HR(rest) + 20 BPM • Duration • Intermittent bouts 3 to 5 mins, as tolerated • Frequency • 3 to 4 times per day (day 2-3) • Two times per day with increased duration of exercise bouts (beginning on day 4) • Initial activities should be monitored, and symptoms HR, BP recorded
Outpatients • Large-muscle group activities • Moderate intensity: 40 to 60% of VO2 max • At least 30 minutes • Preceded by warm-up and followed by cool-down • At least 3 times weekly • Follow-up supervised group sessions are recommended
Cardiac rehabilitation • Core components • Medical assessment • Nutrition counseling • Risk factor management (lipid, DM, weight, smoking) • Psychosocial management • Activity counseling and exercise training
Outpatients exercise program • Setting a safe upper limit for Intensity • Moderate intensity exercise (40 to 60% VO2max) • Brisk walking, treadmill, cycle, stair-climbing, rowing machine • Initial intensity • 40 to 60% of heart rate reserve • Can be increased to 85% (high intensity) if tolerated • RPE • 11 to 13 (between fairly light to somewhat hard) • Duration may be increased as appropriate after safe activity levels established • Intensity may be increased as heart rate response to exercise decreases with conditioning
Exercise prescription without exercise test • Initial exercise intensity • 2 to 3 METs • 1 to 2 mph, 0% grade on treadmill • 100 to 300 kg.m.min-1 (12.5- 50W) on cycle ergometer • RPE: 11-13 • Gradual increments of 0.5 to 1.0 METs as tolerated • Target heart rate • 20 beats/min above standing rest • Frequency • 30 – 45 minutes per day 5 d/wk,
Exercise prescription in the presence of ischemia • Inappropriate for those with angina < 3METS • Aim to increase anginal threshold • Prolonged warm up and cool • Upper body exercises may precipitate angina more readily • Heart rate and work rate below the identified threshold of ischemia • Should be a minimum of 10 beats/min below the heart rate at which the abnormality occurs • Intermittent, shorter duration-type on a more frequent basis
Heart Failure • Benefits of exercise • Functional capacity, improved leg blood flow and oxidative capacity, neurohormones, autonomic tone • Initiated at a low to moderate level (25 to 60% of VO2max) • VO2max determined by direct gas exchange measurements • Careful supervision and monitoring • Brief training session • Lengthened warm up and cool down • RPE: 11 to 14 • Safety and efficacy of resistance training not well established
After cardiac procedure • CABG • Avoid upper body exercise for 3 months • PCI • Resume exercise no sooner than 5 to 7 days • Catheterization access sites should be healed
Pacemakers and implantable cardioverter defibrillators • Type and settings of pacemaker should be noted • Fixed-rate pacemakers • Activity intensity must be gauged by other methods • RPE • ICD • Limit target heart rate at least 10 to 15 beats/min lower than the threshold discharge rate
AHA Scientific Statement: Recommendations for the Acceptability of Recreational (Noncompetitive) Sports Activities and Exercise in Patients With Genetic CVD • GCVD • HCM, LQTS, Marfan syndrome, ARVC, Brugada syndrome • Recreational sports are categorized with regard to high, moderate and low levels of exercise • Graded on relative scale (from 0 to 5) for eligibility • 0 to 1: indicating generally not advised or strongly discouraged • 4 to 5: indicating probably permitted • 2 to 3: indicating intermediate and to be assessed clinically in an individual basis
Intensity Level HCM LQTS Marfan Syndrome ARVC Brugada Symdrome High Basketball 0 0 2 1 2 Full court 0 0 2 1 2 Half court 1 1 0 1 1 Body building 0 0 1 0 0 Ice hockey 0 2 2 0 2 Racquetball/squash 1 1 1 1 1 Rock climbing 0 0 2 0 2 Running (downhill) 2 2 2 1 1 Skiing (cross-country) 2 3 2 1 4 Soccer 0 0 2 0 2 Tennis (singles) 0 0 3 0 2 Touch (flag) football 1 1 3 1 3 Windsurfing 1 0 1 1 1 AHA Scientific Statement: Recommendations for the Acceptability of Recreational (Noncompetitive) Sports Activities and Exercise in Patients With GCVDs Recommendations for Physical Activity and Recreational Sports Participation for Young Patients with Genetic Cardiovascular Diseases, Circulation. 2004; 109:2807-2816)
Intensity Level HCM LQTS Marfan Syndrome ARVC Brugada Symdrome Moderate Baseball/softball 2 2 2 2 4 Biking 4 4 3 2 5 Modest hiking 4 5 5 2 4 Motocycling 3 1 2 2 2 Jogging 3 3 3 2 5 Sailing 3 3 2 2 4 Surfing 2 0 1 1 1 Swimming (lap) 5 0 3 3 4 Tennis (doubles) 4 4 4 3 4 Treadmill/stationary bicycle 5 5 4 3 5 Weightlifting (free weights) 1 1 0 1 1 Hiking 3 3 3 2 4 AHA Scientific Statement: Recommendations for the Acceptability of Recreational (Noncompetitive) Sports Activities and Exercise in Patients With GCVDs Recommendations for Physical Activity and Recreational Sports Participation for Young Patients with Genetic Cardiovascular Diseases, Circulation. 2004; 109:2807-2816)
Intensity Level HCM LQTS Marfan Syndrome ARVC Brugada Symdrome Low Bowling 5 5 5 4 5 Golf 5 5 5 4 5 Horseback riding 3 3 3 3 3 Scuba diving 0 0 0 0 0 Skating 5 5 5 4 5 Snorkeling 5 0 5 4 4 Weights (non-free weights) 4 4 0 4 4 Brisk walking 5 5 5 5 5 AHA Scientific Statement: Recommendations for the Acceptability of Recreational (Noncompetitive) Sports Activities and Exercise in Patients With GCVDs Recommendations for Physical Activity and Recreational Sports Participation for Young Patients with Genetic Cardiovascular Diseases, Circulation. 2004; 109:2807-2816)
Recommendation • Health professionals should personally engage in an active lifestyle Thank You!
References • Exercise standards for testing and training: a statement for healthcare professionals from the American Heart Association. Circulation. 2001;104:1694-1740 • Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: AHA scientific statement. Circulation. 2003;107:3109-3116 • Recommendations for Physical Activity and Recreational Sports Participation for Young Patients with Genetic Cardiovascular Diseases, Circulation. 2004; 109:2807-2816 • ACSM’s guidelines for exercise testing and prescription. 7th edition • 36th Bethesda Conference. Eligibility recommendations for competitive athletes with cardiovascular abnormalities. JACC 19 April 2005 • Recommendations for preparticipation screening and the assessment of cardiovascular disease in masters athletes. Circulation. 2001;103:327-334.