Download
1 / 50
500 likes | 730 Views
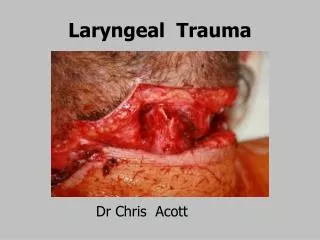
Laryngeal Trauma. Dr Chris Acott. Dr Russell M Davies 1914 - 1991. BMJ July 24 1880 pp 123. Sir William MacEwen 1848-1924.

E N D
Laryngeal Trauma Dr Chris Acott
BMJ July 24 1880 pp 123 Sir William MacEwen 1848-1924 “He sat in bed supporting himself with stiffened arms: his head was thrown forwards, and he had the distressed anxiety so characteristic of impending suffocation …. His inspirations were crowing and laboured, and there was a very frequent forced attempt to swallow, attended by extreme pain, … He spoke in a muffled whisper, and confined his answers, when possible, to monosyllables, or substituted signs by head or hand. …”
Laryngeal trauma Penetrating Blunt
Laryngeal Trauma: incidence Rare 1/5000 – 1/137,000 Current Opinion Otolaryngology 2000; 8(6):497-502 1/14,000 – 1/42,000 American Association Oral Maxillofacial Surgeons 2006: 203-214
Laryngeal Trauma: incidence Rare – Why? under reported - paucity of peer reviewed data - American Association Oral Maxillofacial Surgeons 2006: 203-214 Current Opinion Otolaryngology 2000 8(6):497-502 patients die before reaching hospital – not reported in data larynx well protected & flexible mandible - superiorly; sternocleidomastoids – laterally; clavicles – inferiorly. American Association Oral Maxillofacial Surgeons 2006: 203-214 Current Opinion Otolaryngology 2000 8(6):497-502
Laryngeal Trauma: Diagnosis DIAGNOSIS OF SUSPICION laryngeal trauma NEEDS to be excluded diagnosis may not be obvious in a patient with an uncompromised airway symptoms & signs unrelated to degree of trauma this may also be reason for under reporting Once diagnosed the extent of injury must be defined before any attempt at intubation ETT across injured larynx can convert mucosal laceration to a more complex problem ETT can cause complete laryngo-tracheal separation
Laryngeal Trauma: Morbidity/mortality Mortality 0-18% J Trauma 1990 30(1):87-93 Delay in diagnosis increases morbidity & mortality pharyngeal, oesophageal & vessel injury must be excluded Concurrent occult oesophageal injury significantly contributes to morbidity & mortality evaluation of oesophagus mandatory - NB before placement N/G tube
Laryngeal trauma:Diagnosis of Suspicion • HISTORY • Hoarseness - 90% • Tenderness - 90% • Subcutaneous emphysema - 60% • Anterior neck contusion - 40% • SOB - 40% Current Opinion Otolaryngology 2000 8(6):497-502
Laryngeal trauma:Diagnosis of Suspicion • Inability supine - 30% • Pain - 30% • Tracheal deviation - 20% • Haemoptypsis - 20% • Dysphagia - 10% • Aphonia - 10% Current Opinion Otolaryngology 2000 8(6):497-502
Associated injuries • Chest trauma - 40% • Facial #s - 30% • Facial laceration - 30% • Long Bone #s - 30% • Oesophageal laceration - 10% • Head injury - 10% • Pharyngeal trauma/perforation - rare • None - 30% Current Opinion Otolaryngology 2000 8(6):497-502
Laryngeal trauma:History may give some idea of injury • Complete L-T separation associated with: • hyperextension injuries: avulsion of larynx – tearing of fibrous ring between CC & 1st tracheal ring • strangulation • rarely associated with blunt trauma • ASSOCIATED WITH # CRICOID CARTILAGE • # Thyroid Cartilage: • neck hyperflexion • Knife or Gunshot wounds • evaluate the oesophagus
Multiple threats to airway: • Direct penetration • Distorted tissue planes • Haematoma • Oedema • Excessive blood & secretions
Multiple threats to airway: ..2 • IPPV & coughing: • worsen air leaks • s/c emphysema • Cricoid pressure: • lead to laryngo-tracheal separation
Multiple threats to airway: ..3 • Cricothyroidotomy: • may compound injury • ETT: • mucosal disruption • false passage • laryngo-tracheal separation
Laryngeal trauma: Airway Unstable Stable Airway can become unstable at anytime
Laryngeal trauma: Airway Unstable Stable Inability to tolerate supine position – URGENT TRACHEOSTOMY
Vocal cord injury Arytenoid swelling & dislocation Crico-tracheal separation usually associated with death Soft tissue contusion Superficial mucosal laceration Laryngeal Injuries: ..1
Laryngeal Injuries: …2 • Thyroid cartilage fracture • most common site of fracture • Epiglottic fracture • Mixed injuries • Shattered calcified thyroid cartilage in elderly
Investigations: • Plain Xray (may not be helpful due to extensive s/c emphysema) • pneumomediastinum & pneumothorax • air in tissues • # Cx spine • CT • cartilage & soft tissue injury • airway patency
Investigations: .2 • Laryngoscopy • vocal cord paralysis • mucosal & cartilage separation • haematoma • Laceration • Arytenoid displacement
Fractured Larynx:Management • Tracheostomy under LA vs GA • Management is NOT A LEARNING EXPERIENCE • HELIOX • FOB & Cricothyroidotomy may not be appropriate • Intubation may not be appropriate • may cause complete separation
WHY HELIOX? Less dense – work of breathing less. Decrease amount of subcutaneous emphysema
Helium - Upper airway obstruction “When it is available an even better effect can be expected from inhalation of 79% Helium with 21% Oxygen” Wylie Churchill Davidson 1960 pp 382
Reynold’s Number < 2000 laminar flow 2000 -10000 transitional flow >10000 turbulent flow
Turbulent flow Turbulent flow F ~ P1/2/Lρ1/2 F = flow; P = pressure; ρ = density; L = length. (Radius important but not expressible as a power of the diameter - as radius decreases flow decreases also) Turbulent flow: flow greater with Heliox than air or O2 Density important
Relationship between pressure and flow during turbulent flow Even if flow is turbulent there is less work of breathing and greater flow with given pressure change Heliox O2 Comparison between Heliox (black) & air or O2 (yellow)
Why Helium?Hylegaard et al • O2 breathing initial bubble growth • O2 > He solubility in fat • build up O2 around bubble in tissue • Helium breathing bubble constantly shrunk
Helium mixtures:Physics /Gas flux • GAS FLUX = diffusion x solubility coefficient • He>N2 diffusibility (smaller atomic wt) • He<N2 solubility in fatty tissue, water & blood • He<O2 solubility in fatty tissue • therefore:- • N2 or O2 flux into fatty tissue > He flux HENSE ANY AIR POCKETS WILL SHRINK.
WHY HELIOX? • HELIOX WILL GAIN PATIENT’S CONFIDENCE AND MAKE BREATHING EASIER • AND MAY DECREASE THE AMOUNT OF S/C EMPHYSEMA.
5 Case Histories Maybe others – but not recognised. • trauma patients on ICU ventilator – laryngeal oedema when extubated a couple of days later – ‘floppy epiglottis’ on intubation 1. Walker in mountains • hoarse voice in GP’s surgery • GA - laryngoscopy – unable to identify any structures, unable to intubate (fortunately!!) • obstructed during tracheostomy with retractors 2. Motorcyclist on farmer’s property • intubated at scene
5 Case Histories 3. MVA – car rolled. • hanged by seat belt upside down • complete tracheal/laryngeal separation • partial obstruction with palpation of neck - GA 4. Motorcyclist – MVA – Modbury Hospital • gaseous induction • complete obstruction during tracheostomy – retractors again 5. And ….
Able to speak and say “EEEE” • Air bubbling freely from thyroid holes • covered with wet drape • CT scan –no # Cricoid!! • found to have one • No s/c emphysema • No respiratory distress • Able to lie flat
SURGICAL TRACHEOSTOMY Head extended exposing the neck. Neck palpated. LA injected. May not be able to extend the head. Palpation of structures may press on trachea & cause anxiety. LA stings – may increase anxiety. Horizontal 6 cm incision to anterior borders sternocleidomastoid muscles. Skin, subcut tissue, platysma to deep fascia. Veins may be enlarged due to inspiratory/expiratory pressures
Self retaining retractor placed, dissection to strap muscles Strap muscles divided & retracted. Langerbech retractors placed. Retractor placement important – to much pressure can obstruct airway.
Thyroid isthmus exposed, clamped , divided and ligated, rotated externally & sutured. Retractor placement again important – to much pressure can obstruct airway. Trachea is exposed
Tracheal incision sited over 2nd & 3rd or 3rd & 4th tracheal rings. Tracheostomy tube inserted Placement of tube may cause some distress
Summary: • Rare – diagnosis of suspicion • Mortality ~20% • increases if unrecognised • Concurrent oesophageal injury increases morbidity & mortality • needs to be excluded • Inability to lie supine – indication immediate tracheostomy
Summary: ..2 • Consider Heliox if available • Avoid coughing – may make s/c emphysema worse and airway impossible • Awake tracheostomy vs SV GA? • careful palpation • care with retractors
3rd SIG Airway MeetingLorne March 9-11 2012“Everything airways including problems outside the OT”
Laryngeal Trauma Dr Chris Acott
Head extended exposing the neck.** Neck palpated. LA injected.* Horizontal 6 cm incision. Anterior borders sternocleidomastoid muscles. Skin, subcut tissue, platysma to deep fascia. Self retaining retractor placed, dissection to strap muscles.* Strap muscles divided & retracted. Langerbech retractors placed.**
Thyroid Isthmus divided. Trachea is exposed Sited over 2nd& 3rdor 3rd& 4th tracheal rings